

Ocular Manifestations of Hurler-Scheie Syndrome: Recurrence of Host Disease in the Corneal Transplant
- PMID: 36777710
- PMCID: PMC9911992
- DOI: 10.1159/000525453
Ocular Manifestations of Hurler-Scheie Syndrome: Recurrence of Host Disease in the Corneal Transplant
Abstract
Introduction: Hurler-Scheie syndrome is a type of mucopolysaccharidosis I (MPS). In MPS I the decreased activity of alpha-L-iduronidase lysosomal enzyme leads to glycosaminoglycan (GAG) deposition in the intra- and extracellular matrix. Excessive amounts of GAG can accumulate in most layers of the cornea, including epithelial cells, stromal keratocytes, and endothelial cells.
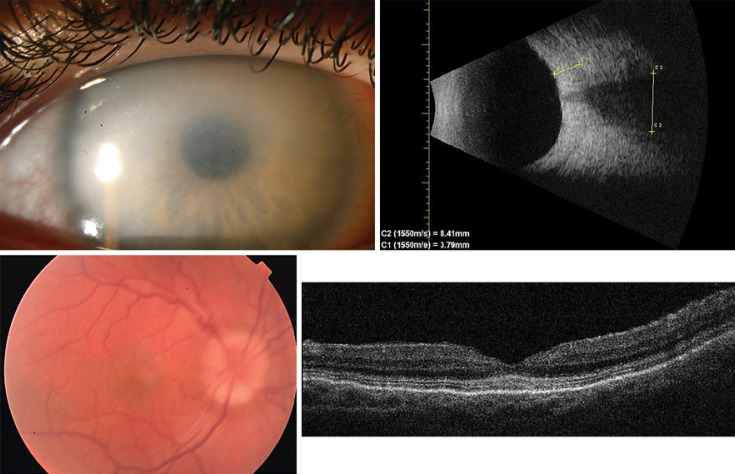
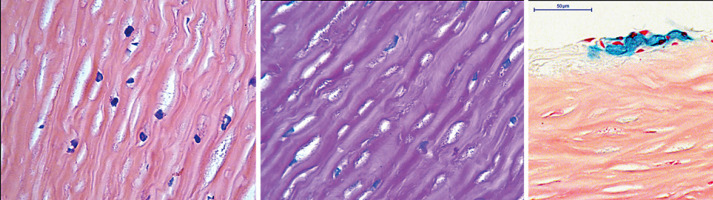
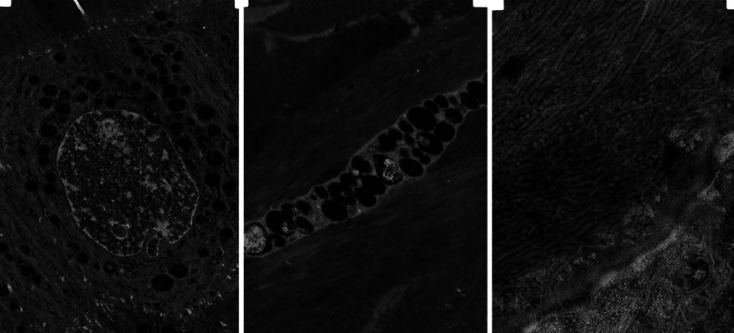
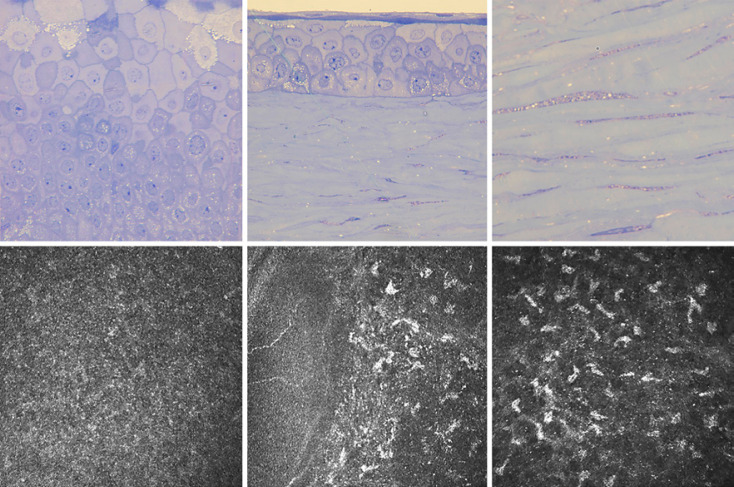
Case presentation: A 25-year-old female patient suffering from Hurler-Scheie syndrome with multiple ocular manifestations is reported. Due to significant bilateral corneal opacification, penetrating keratoplasty was performed on both eyes. Histopathologic examination of the corneal buttons showed disorganized collagen fibers with heterogenous thickness and many granule-containing keratocytes with excessive cytoplasm. Despite receiving enzyme replacement therapy, in vivo confocal microscopy revealed characteristic vacuoles in the basal epithelium and corneal stroma 96 months after transplantation. High resolution anterior segment optical coherence tomography demonstrated hyperreflective opacities superficial and deeper in the stroma which was consistent with recurrence of host disease in the graft.
Conclusion: To the best of our knowledge, this is the first documented Hurler-Scheie syndrome case of recurrence after penetrating keratoplasty demonstrated by in vivo confocal microscopy. Additionally, this patient manifested severe ocular involvement of MPS which might be an explanation of the progressive course of corneal opacification after transplantation.
Keywords: Hurler-Scheie syndrome; In vivo confocal microscopy; Lysosomal storage disease; Mucopolysaccharidosis; Recurrence.
Copyright © 2022 by The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Multimodal imaging of Hurler syndrome-related keratopathy treated with deep anterior lamellar keratoplasty.BMC Ophthalmol. 2020 Oct 31;20(1):433. doi: 10.1186/s12886-020-01689-2. BMC Ophthalmol. 2020. PMID: 33129306 Free PMC article.
-
Anterior segment optical coherence tomography and in vivo confocal microscopy in cases of mucopolysaccharidosis.Am J Ophthalmol Case Rep. 2020 Apr 30;19:100728. doi: 10.1016/j.ajoc.2020.100728. eCollection 2020 Sep. Am J Ophthalmol Case Rep. 2020. PMID: 32405572 Free PMC article.
-
Progressive eye pathology in mucopolysaccharidosis type I mice and effects of enzyme replacement therapy.Clin Exp Ophthalmol. 2020 Apr;48(3):334-342. doi: 10.1111/ceo.13713. Epub 2020 Jan 30. Clin Exp Ophthalmol. 2020. PMID: 31925897
-
[Mucopolysaccharidosis type I, Hurler-Scheie phenotype with ocular involvement. Clinical and ultrastructural study].J Fr Ophtalmol. 1994;17(4):286-95. J Fr Ophtalmol. 1994. PMID: 8089412 Review. French.
-
Mucopolysaccharidosis type I.Pediatr Endocrinol Rev. 2014 Sep;12 Suppl 1:102-6. Pediatr Endocrinol Rev. 2014. PMID: 25345091 Review.
References
-
- Aragona P, Wylegala E, Wroblewska-Czajka E, Smedowski A, Nowinska A, Roszkowska AM, et al. Clinical, confocal, and morphological investigations on the cornea in human mucopolysaccharidosis IH-S. Cornea. 2014;33:35–42. - PubMed
-
- Ashworth JL, Biswas S, Wraith E, Lloyd IC. Mucopolysaccharidoses and the eye. Surv Ophthalmol. 2006a;51:1–17. - PubMed
-
- Ashworth JL, Biswas S, Wraith E, Lloyd IC. The ocular features of the mucopolysaccharidoses. Eye (Lond) 2006b;20:553–563. - PubMed
-
- Bothun ED, Decanini A, Summers CG, Orchard PJ, Tolar J. Outcome of penetrating keratoplasty for mucopolysaccharidoses. Arch Ophthalmol. 2011;129:138–144. - PubMed
-
- Davson H. The Eye. Orlando: Academic Press; 1984.
Publication types
LinkOut - more resources
Full Text Sources
