

Efficacy, Safety, and Reliability of the Single Anterior Approach for Subaxial Cervical Spine Dislocation
- PMID: 36777970
- PMCID: PMC9909243
- DOI: 10.7759/cureus.34787
Efficacy, Safety, and Reliability of the Single Anterior Approach for Subaxial Cervical Spine Dislocation
Abstract
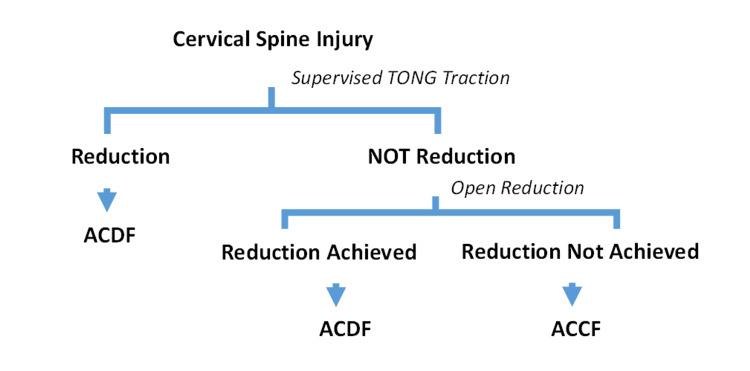
Background Though there is ongoing controversy regarding the best treatment option for cervical spine dislocation (CSD), anterior cervical surgery with direct decompression is becoming widely accepted. However, managing all cases of subaxial CSD entirely by a single anterior approach is rarely seen in the published literature. Methods The study comprised patients with subaxial CSD who underwent surgical stabilization utilizing a single anterior approach. Most of the CSD was reduced and anterior cervical discectomy and fusion (ACDF) were performed. Anterior cervical corpectomy and fusion (ACCF) were done in unreduced dislocations. The patient's neurological condition, radiological findings, and functional outcomes were assessed. SPSS version 25.0 (IBM Corp., Armonk, NY) was used for statistical analysis. Results The total number of operated cases was 64, with an average of 42 months of follow-up. The mean age was 34.50±11.92 years. The most prevalent level of injury was C5/C6 (57.7%). Reduction was achieved in 92.2% of cases; only 7.8% of patients needed corpectomy. The typical operative time was 84.25±9.55 minutes, with an average blood loss of 112.12±25.27 ml. All cases except complete spinal cord injury (CSI) were improved neurologically (87.63%). The mean Neck Disability Index (NDI) was 11.14±11.43, and the pre-operative mean visual analog score (VAS) was finally improved to 2.05±0.98 (P<0.05). In all cases, fusion was achieved. The most common complication was transient dysphagia (23.4%). After surgery, no patient developed or aggravated a neurological impairment. Implant failure was not observed at the final follow-up except for two cases where screws were pulled out partially. Conclusion Based on the results of this study, a single anterior approach is a safe and effective procedure for subaxial CSD treatment with favorable radiological, neurological, and functional outcomes.
Keywords: anterior cervical corpectomyand fusion (accf); anterior cervical discectomy and fusion (acdf); single anterior approach; subaxial cervical spine dislocation (csd); traumatic cervical spine injury.
Copyright © 2023, Jonayed et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Comparative study of surgical approaches for distractive flexion injuries of the sub-axial cervical spine. Al Samouly HM, Taha AM. Open J Mod Neurosurg. 2018;8:342–351.
-
- Treatment of traumatic dislocations of the cervical spine through anterior approach. Defino HL, Figueira FG, Camargo LS, Canto FR. https://www.scielo.br/j/aob/a/LSrMTwBG69CWPQZC9p4rwZR/?format=pdf&lang=en Acta Ortop Bras. 2007;15:30–34.
-
- Controversies in the treatment of cervical spine dislocations. Lee JY, Nassr A, Eck JC, Vaccaro AR. Spine J. 2009;9:418–423. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous