

This is a preprint.
Machine Learning for the ECG Diagnosis and Risk Stratification of Occlusion Myocardial Infarction at First Medical Contact
- PMID: 36778371
- PMCID: PMC9915770
- DOI: 10.21203/rs.3.rs-2510930/v1
Machine Learning for the ECG Diagnosis and Risk Stratification of Occlusion Myocardial Infarction at First Medical Contact
Update in
-
Machine learning for ECG diagnosis and risk stratification of occlusion myocardial infarction.Nat Med. 2023 Jul;29(7):1804-1813. doi: 10.1038/s41591-023-02396-3. Epub 2023 Jun 29. Nat Med. 2023. PMID: 37386246 Free PMC article.
Abstract
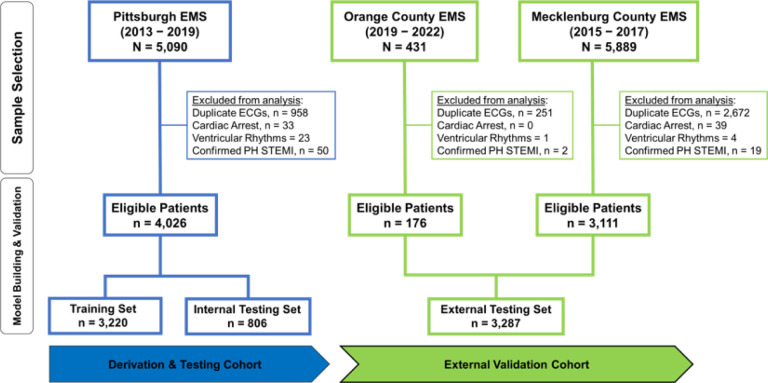
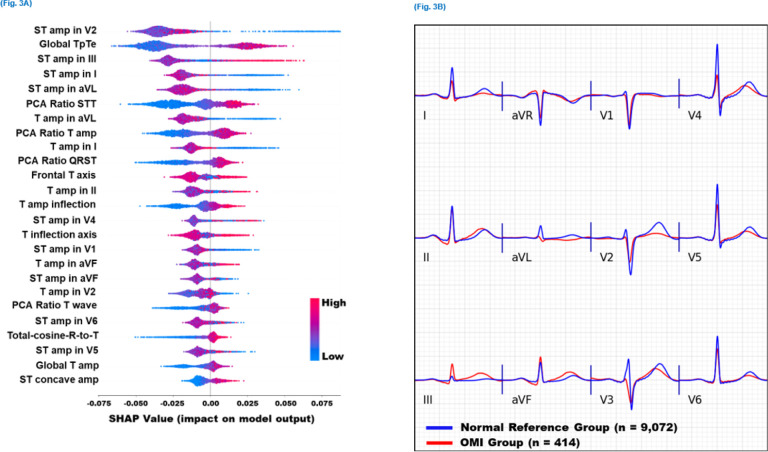
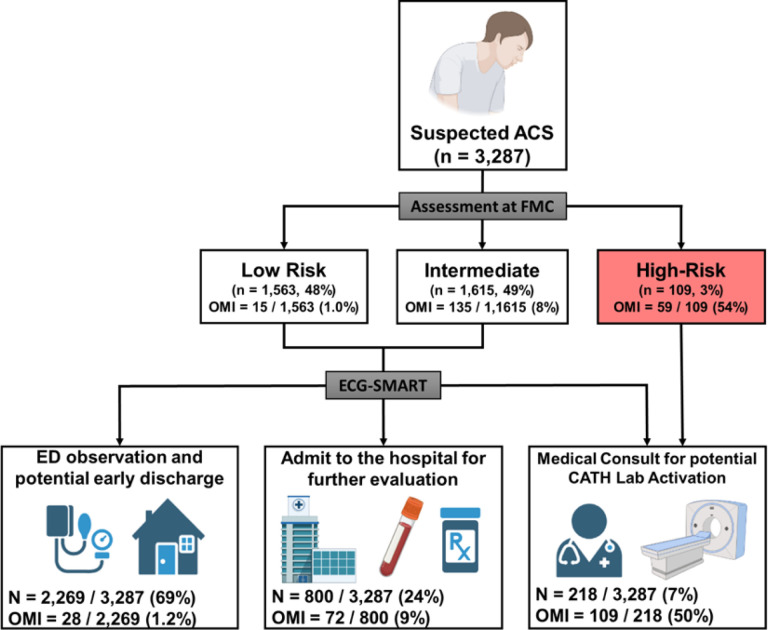
Patients with occlusion myocardial infarction (OMI) and no ST-elevation on presenting ECG are increasing in numbers. These patients have a poor prognosis and would benefit from immediate reperfusion therapy, but we currently have no accurate tools to identify them during initial triage. Herein, we report the first observational cohort study to develop machine learning models for the ECG diagnosis of OMI. Using 7,313 consecutive patients from multiple clinical sites, we derived and externally validated an intelligent model that outperformed practicing clinicians and other widely used commercial interpretation systems, significantly boosting both precision and sensitivity. Our derived OMI risk score provided superior rule-in and rule-out accuracy compared to routine care, and when combined with the clinical judgment of trained emergency personnel, this score helped correctly reclassify one in three patients with chest pain. ECG features driving our models were validated by clinical experts, providing plausible mechanistic links to myocardial injury.
Conflict of interest statement
DECLARATION OF INTERESTS
US Patent # 10820822, Owner: University of Pittsburgh, Inventors: SSA, ES, and CWC.
Figures


References
-
- Goodacre S, Pett P Arnold J, et al. Clinical diagnosis of acute coronary syndrome in patients with chest pain and a normal or non-diagnostic electrocardiogram. Emergency medicine journal. 2009;26(12):866–870. - PubMed
-
- Boubaker H, Grissa MH, Beltaief K, et al. A new score for the diagnosis of acute coronary syndrome in acute chest pain with non-diagnostic ECG and normal troponin. Emergency Medicine Journal. 2015;32(10):764–768. - PubMed
-
- Ioannidis JP Salem D, Chew PW, Lau J. Accuracy and clinical effect of out-of-hospital electrocardiography in the diagnosis of acute cardiac ischemia: a meta-analysis. Annals of emergency medicine. 2001;37(5):461–470. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
