

Patient Outcomes and Unit Composition With Transition to a High-Intensity ICU Staffing Model: A Before-and-After Study
- PMID: 36778910
- PMCID: PMC9904765
- DOI: 10.1097/CCE.0000000000000864
Patient Outcomes and Unit Composition With Transition to a High-Intensity ICU Staffing Model: A Before-and-After Study
Abstract
Provider staffing models for ICUs are generally based on pragmatic necessities and historical norms at individual institutions. A better understanding of the role that provider staffing models play in determining patient outcomes and optimizing use of ICU resources is needed.
Objectives: To explore the impact of transitioning from a low- to high-intensity intensivist staffing model on patient outcomes and unit composition.
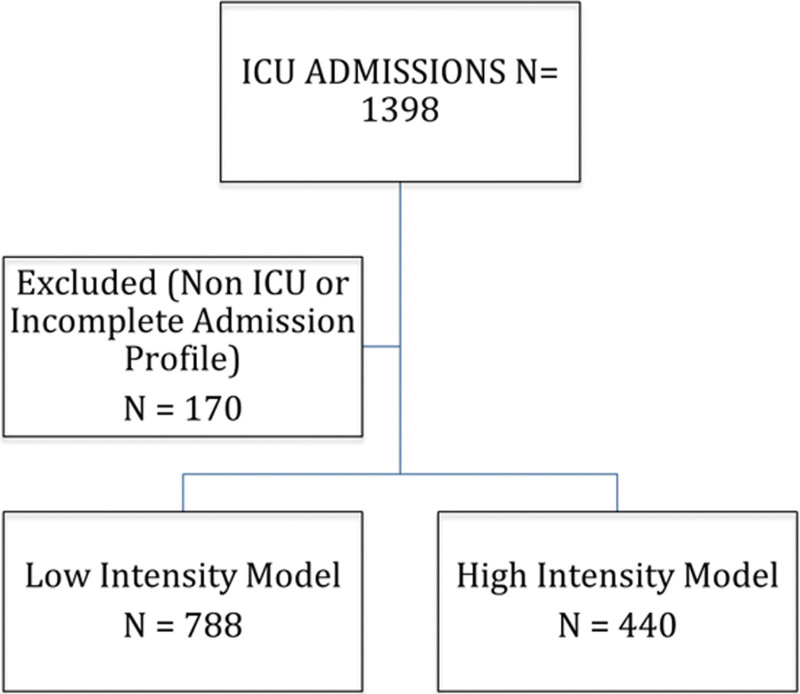
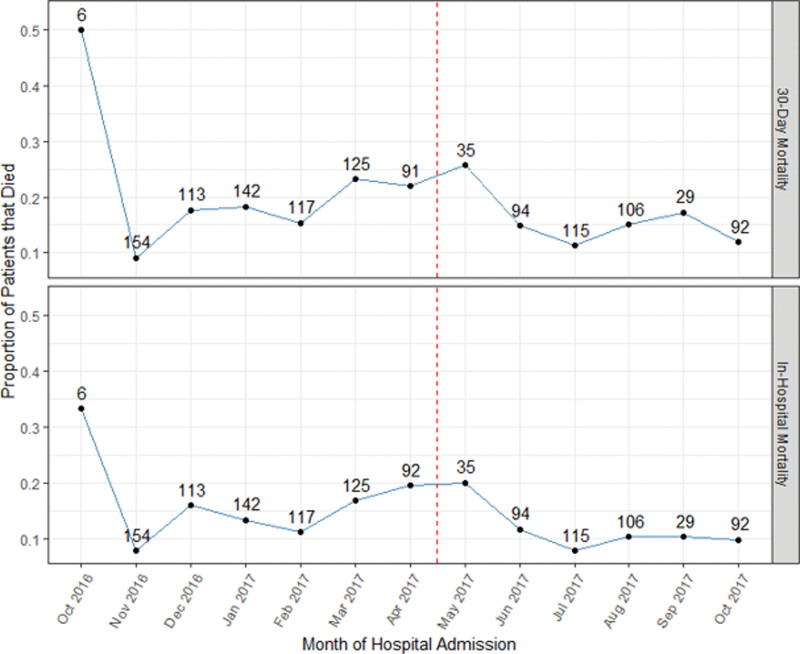
Design setting and participants: This was a prospective observational before-and-after study of adult ICU patients admitted to a single community hospital ICU before (October 2016-May 2017) and after (June 2017-November 2017) the transition to a high-intensity ICU staffing model.
Main outcomes and measures: The primary outcome was 30-day all-cause mortality. Secondary outcomes included in-hospital mortality, ICU length of stay (LOS), and unit composition characteristics including type (e.g., medical, surgical) and purpose (ICU-specific intervention vs close monitoring only) of admission.
Results: For the primary outcome, 1,219 subjects were included (779 low-intensity, 440 high-intensity). In multivariable analysis, the transition to a high-intensity staffing model was not associated with a decrease in 30-day (odds ratio [OR], 0.90; 95% CI, 0.61-1.34; p = 0.62) or in-hospital (OR, 0.89; 95% CI, 0.57-1.38; p = 0.60) mortality, nor ICU LOS. However, the proportion of patients admitted to the ICU without an ICU-specific need did decrease under the high-intensity staffing model (27.2% low-intensity to 17.5% high-intensity; p < 0.001).
Conclusions and relevance: Multivariable analysis showed no association between transition to a high-intensity ICU staffing model and mortality or LOS outcomes; however, the proportion of patients admitted without an ICU-specific need decreased under the high-intensity model. Further research is needed to determine whether a high-intensity staffing model may lead to more efficient ICU bed usage.
Keywords: hospital mortality; intensive care unit; intensive care unit triage; intensivist staffing; length of stay.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Angus DC, Shorr AF, White A, et al. : Critical care delivery in the United States: Distribution of services and compliance with Leapfrog recommendations. Crit Care Med 2006; 34:1016–1024 - PubMed
-
- Garland A, Gershengorn HB: Staffing in ICUs: Physicians and alternative staffing models. Chest 2013; 143:214–221 - PubMed
-
- Holdorf JD, Lilly CM: Intensivist staffing: Evolving challenges and solutions. Semin Respir Crit Care Med 2015; 36:842–850 - PubMed
LinkOut - more resources
Full Text Sources
