

Higher Dose Oral Fluconazole for the Treatment of AIDS-related Cryptococcal Meningitis (HIFLAC)-report of A5225, a multicentre, phase I/II, two-stage, dose-finding, safety, tolerability and efficacy randomised, amphotericin B-controlled trial of the AIDS Clinical Trials Group
- PMID: 36780493
- PMCID: PMC9925064
- DOI: 10.1371/journal.pone.0281580
Higher Dose Oral Fluconazole for the Treatment of AIDS-related Cryptococcal Meningitis (HIFLAC)-report of A5225, a multicentre, phase I/II, two-stage, dose-finding, safety, tolerability and efficacy randomised, amphotericin B-controlled trial of the AIDS Clinical Trials Group
Abstract
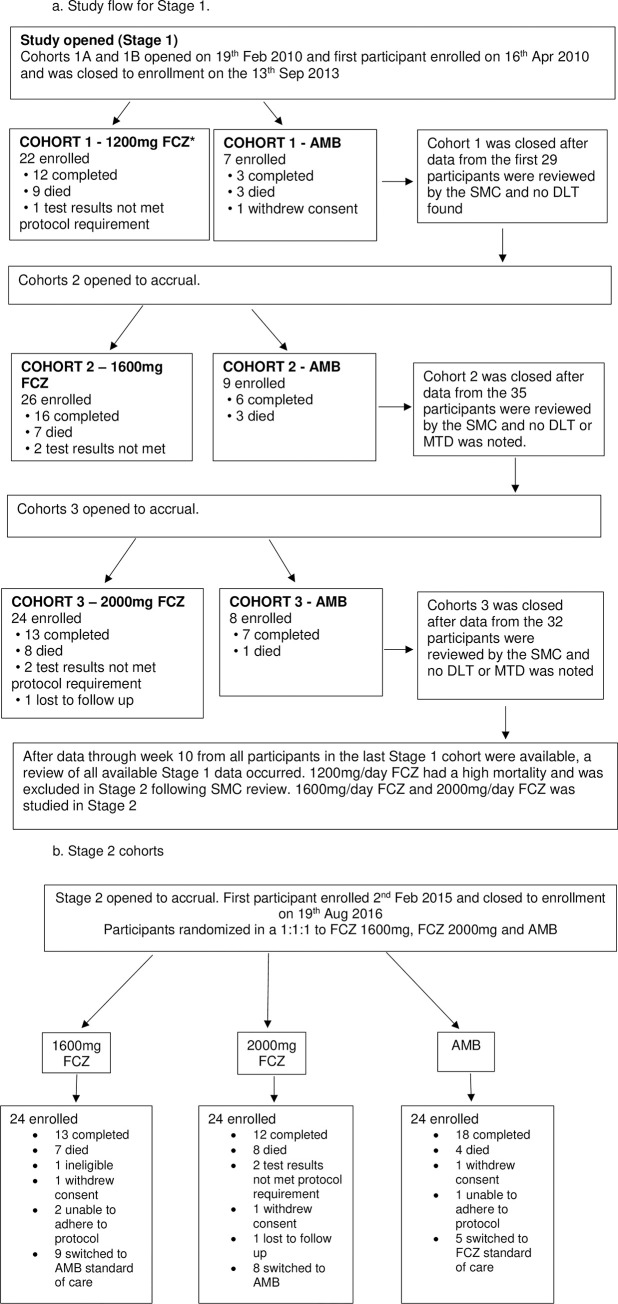
Background: The WHO recommended 1200mg/day of fluconazole (FCZ) in the induction phase of cryptococcal meningitis (CM) in HIV prior to 2018 in regions where amphotericin-B (AMB) was unavailable. A 2-stage AMB-controlled, dose-escalation study to determine the maximum tolerated dose and the safety/efficacy of an induction-consolidation strategy of higher doses FCZ (1200mg-2000mg/day), adjusted for weight and renal function (eGFR)in adults with CM was undertaken.
Methods: In Stage-1, three induction doses of FCZ (1200mg/day, 1600mg/day and 2000mg/day) were tested in sequential cohortsand compared with AMB in a 3:1 ratio. A particular dose was not tested in Stage 2 if there were significant predetermined safety or efficacy concerns. In Stage-2, the 1200mg dose was excluded per protocol because of increased mortality, and participants were randomised to 1600mg, 2000mg FCZ or AMB in a 1:1:1 ratio.
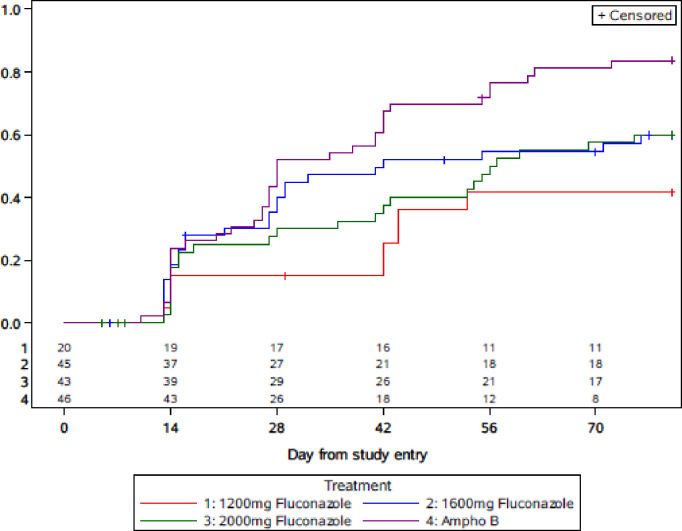
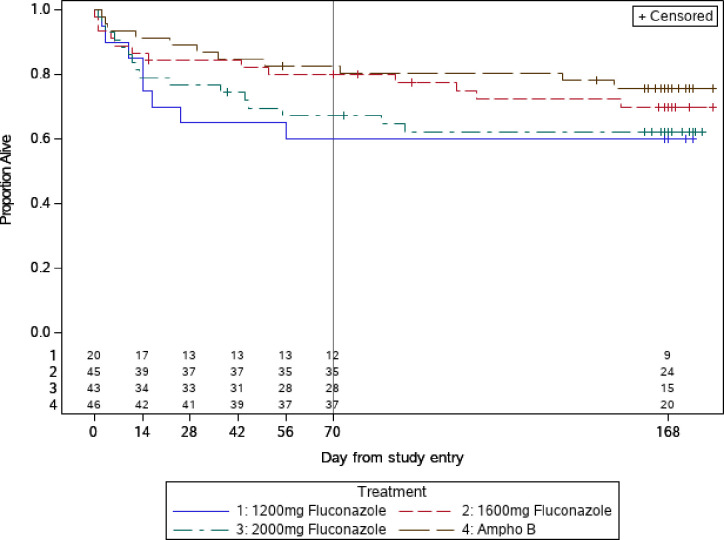
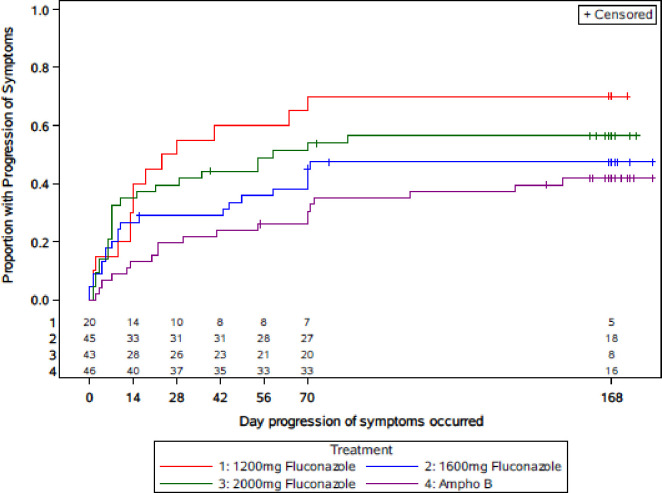
Findings: One hundred and sixty eight participants were enrolled with 48, 50, and 48 in the AMB, 1600mg and 2000mg cohorts. The Kaplan Meier proportion for mortality (90% CI) at 10 and 24 weeks for AMB was 17% (10, 29) and 24% (15, 37), compared to 20% (12, 32) and 30% (20, 43) for 1600mg, and 33% (23, 46) and 38% (27, 51) for 2000mg/day FCZ. With the exception of a higher incidence of gastrointestinal side effects in the 2000mg cohort, both induction doses of FCZ were safe and well tolerated. There were no life-threatening changes in electrocardiogram QTc which were similar across all doses of FCZ and AMB. The median (IQR) change in log10 cryptoccal colony forming units (CFU) from week 0 to week 2 was -8(-4.1,-1.9) for AMB; -2.5(-4.0, -1.4) for 1600mg FCZ and -8 (-3.2, -1.0) for 2000mg FCZ. The proportion (90% CI) CSF CM negative at 10 weeks was 81%(71,90) for AMB; 56%(45,69) for 1600mg FCZ and 60%(49,73) for 2000mg FCZ.
Interpretation: Induction phase weight and renal-adjusted doses of 1600mg and 2000mg/day FCZ for CM were safe and well tolerated except for increased GI side effects in the 2000mg/day dose, and had similar times to achieve CSF sterilization, but took significantly longer than AMB. The WHO recommended 1200mg FCZ was associated with a high mortality. While not statistically significant, mortality was numerically lower in the AMB compared to 1600mg and 2000mg FCZ These data make a case for a phase 3 study of higher doses of FZC.
Trial registration: ClinicalTrials.gov NCT00885703.
Copyright: © 2023 Lalloo et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf. Accessed January 22, 2018.
-
- Nussbaum JC, Jackson A, Namarika D, Phulusa J, Kenala J, Kanyemba C, et al.. Combination flucytosine and high dose fluconazole compared with fluconazole monotherapy for the treatment of cryptococcal meningitis: a randomized trial in Malawi. Clin Infect Dis 2010;50:338–344. doi: 10.1086/649861 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
