

Prevalence, outcomes and costs of a contemporary, multinational population with heart failure
- PMID: 36781285
- PMCID: PMC10086499
- DOI: 10.1136/heartjnl-2022-321702
Prevalence, outcomes and costs of a contemporary, multinational population with heart failure
Abstract
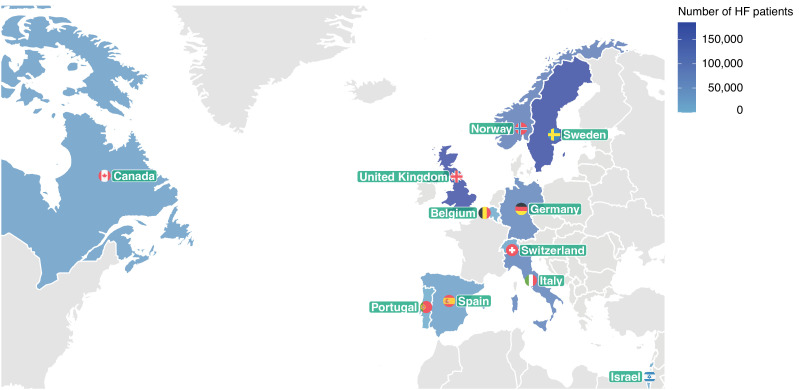
Objective: Digital healthcare systems could provide insights into the global prevalence of heart failure (HF). We designed the CardioRenal and Metabolic disease (CaReMe) HF study to estimate the prevalence, key clinical adverse outcomes and costs of HF across 11 countries.
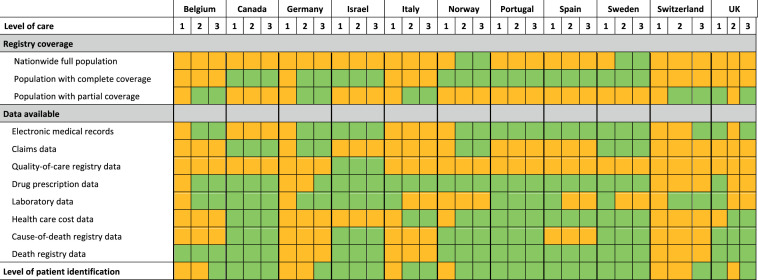
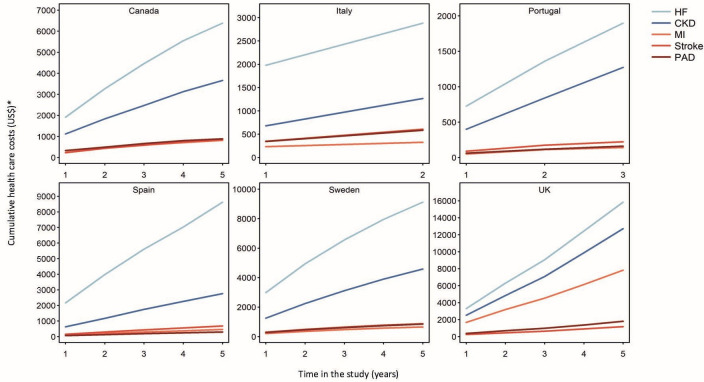
Methods: Individual level data from a contemporary cohort of 6 29 624 patients with diagnosed HF was obtained from digital healthcare systems in participating countries using a prespecified, common study plan, and summarised using a random effects meta-analysis. A broad definition of HF (any registered HF diagnosis) and a strict definition (history of hospitalisation for HF) were used. Event rates were reported per 100 patient years. Cumulative hospital care costs per patient were calculated for a period of up to 5 years.
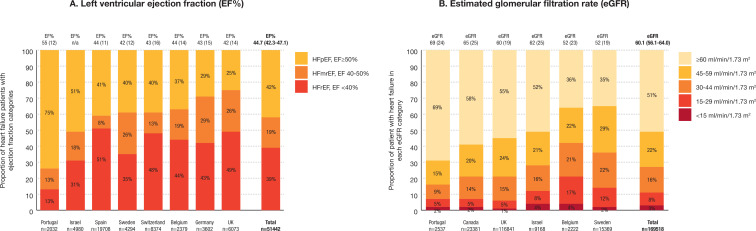
Results: The prevalence of HF was 2.01% (95% CI 1.65 to 2.36) and 1.05% (0.85 to 1.25) according to the broad and strict definitions, respectively. In patients with HF (broad definition), mean age was 75.2 years (95% CI 74.0 to 76.4), 48.8% (40.9-56.8%) had ischaemic heart disease and 34.5% (29.4-39.6%) had diabetes. In 51 442 patients with a recorded ejection fraction (EF), 39.1% (30.3-47.8%) had a reduced, 18.8% (13.5-24.0%) had a mildly reduced and 42.1% (31.5-52.8%) had a preserved left ventricular EF. In 1 69 518 patients with recorded estimated glomerular filtration rate, 49% had chronic kidney disease (CKD) stages III-V. Event rates were highest for cardiorenal disease (HF or CKD) and all cause mortality (19.3 (95% CI 11.3 to 27.1) and 13.1 (11.1 to 15.1), respectively), and lower for myocardial infarction, stroke and peripheral artery disease. Hospital care costs were highest for cardiorenal diseases.
Conclusions: We estimate that 1-2% of the contemporary adult population has HF. These individuals are at significant risk of adverse outcomes and associated costs, predominantly driven by hospitalisations for HF or CKD. There is considerable public health potential in understanding the contemporary burden of HF and the importance of optimising its management.
Keywords: Epidemiology; Heart Failure.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AN has received honoraria from MSD, AstraZeneca, Eli Lilly, Boehringer Ingelheim and Novo Nordisk. JB holds a full time position at AstraZeneca as an epidemiologist. NT reports grants and personal fees from AstraZeneca, grants and personal fees from Janssen, grants and personal fees from BI-Lilly, grants and personal fees from Otsuka, grants, personal fees and other from Tricida, personal fees and other from Pulsedata, personal fees and other from Mesentech, personal fees and other from Renibus, and other from ClinPredict, outside the submitted work; NT has a patent for a microfluidic device for point of care detection of urine albumin pending. AK has received research grants and speaking honoraria from Astrazeneca, Novonordisk and Boehringer Ingelheim. APM reports receiving fees for serving on study committees from AstraZeneca, Novartis, Bayer and Fresenius, outside the present work. TT-G declares speaker and consulting fees from AstraZeneca, BIAL, Daiichi-Sankyo, MSD, Medinfar and Novartis; TT-G holds shares in MTG. MB has received honoraria from Astra Zeneca, Janssen, Lilly, Boehringer Ingelheim, Sanofi, Amgen and Novo Nordisk. MT holds a full time position by an independent statistical consultant company, Statisticon AB, Uppsala, Sweden, of which AstraZeneca Nordic is a client. JS reports stock ownership in companies providing services to Itrim, Amgen, Janssen, Novo Nordisk, Eli Lilly, Boehringer, Bayer, Pfizer, Takeda and AstraZeneca, outside the submitted work. AB is supported by research funding from NIHR, British Medical Association, AstraZeneca and UK Research and Innovation. ABo is part of the BigData@Heart Consortium, funded by the Innovative Medicines Initiative-2 Joint Undertaking under grant agreement No 116074; this joint undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA. KAS has received speaking honoraria from Astrazeneca, Novonordisk, Sanofi and Boehringer Ingelheim.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous