

What have we learnt from the past - would treatment decisions for GEP-NET patients differ between 2012 to 2016 by the new recommendations in 2022?
- PMID: 36782152
- PMCID: PMC9926660
- DOI: 10.1186/s12885-023-10567-1
What have we learnt from the past - would treatment decisions for GEP-NET patients differ between 2012 to 2016 by the new recommendations in 2022?
Abstract
Background: Gastroenteropancreatic neuroendocrine tumors (GEP-NETs) are a heterogeneous group of tumors with a broad range of local and systemic treatment options. Still a lack of data regarding treatment sequences exists. The aim of this study was to analyse outcomes in GEP-NETs depending on stage and treatment steps and compare our treatment decisions to the latest treatment recommendations of European Society of Medical Oncology (ESMO) 2020 for GEP-NETs.
Methods: Patients were included in this retrospective single-center analysis from 2012-2016. All patients suffering from a GEP-NET, who were screened, treated or evaluated at ENETS Center in Zurich, Switzerland were included in analysis. Patients with any other diagnosis of NET were not included. We used Kaplan Meier estimator as well as Cox regression to compare survival rates between different sites of localization, grades or stages and treatment sequences.
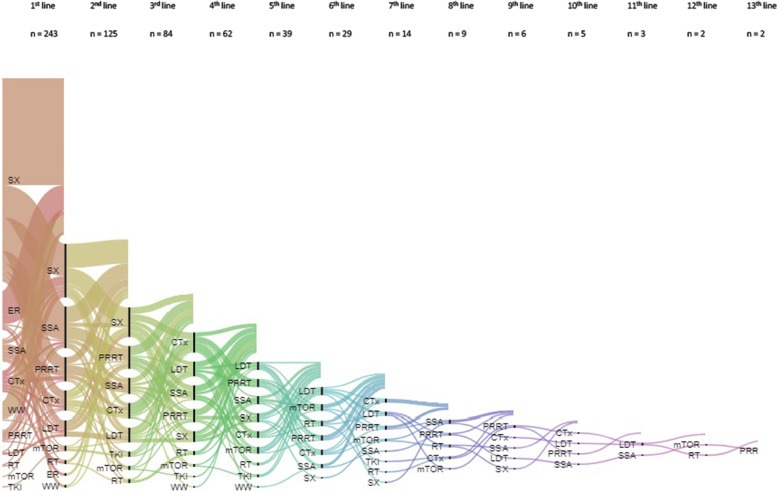
Results: Overall, we identified 256 GEP-NETs, most in advanced stage (62%) and located in small intestine tract or pancreatic gland. Survival depended on stage, grade, primary site and duration of response for the early systemic treatment. On average patients underwent 2.6 different treatment modalities, mostly depending on stage and higher tumor grade. Surgery was performed early but also in advanced stages, usually followed by Somatostatine-Agonist modalities. In distant disease (Stage IV), we investigated a positive effect of PFS after treatment with Somatostatine Analogues (SSA) (hazard ratio [HR], 0.45; 95% confidence interval [CI], 0.21 - 0.97; p = 0.04) and systemic treatment (HR, 0.51; 95% CI, 0.26 - 0.99; p = 0.047) if patients underwent prior surgery or endoscopic resection. Kaplan Meier distributions predict shorter OS in distant disease (Stage IV), (Figure. 1; HR, 2.06; 95% CI, 1.46 - 2.89; log-rank test, p < 0.001).
Conclusion: This retrospective analysis presents a great overview of all patients', disease and treatment characteristics of GEP-NETs at ENETS Center in Zurich, Switzerland. We illustrated survival (PFS) depending on implemented therapies. According to these findings, we formed a suggested treatment algorithm for advanced GEP-NETs, which does not differ from the latest treatment recommendation by ESMO guidelines for GEP-NETs. The results of this project may define GEP-NET patients' selection for upcoming clinical prospective studies.
Keywords: GEP-NET; Overall survival; Progression free survival; Real-life population; SSA; Treatment sequences.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Oncology P. Database Report 2015. 2016. https://www.swissnet.net/images/files/SwissNETReport2015.pdf.
-
- Kollar A, Bütikofer L, Ochsenbein A, Stettler C, Trepp R. Treatment sequence in patients with neuroendocrine tumours: a nationwide multicentre, observational analysis of the Swiss neuroendocrine tumour registry. Swiss Med Wkly. 2020;150:w20176. 10.4414/smw.2020.20176. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
