

Benefits in quality of life following an obstructive sleep apnea screening and treatment program in patients with acute ischemic stroke
- PMID: 36782347
- PMCID: PMC10364071
- DOI: 10.33588/rn.7604.2022359
Benefits in quality of life following an obstructive sleep apnea screening and treatment program in patients with acute ischemic stroke
Abstract
Introduction: Obstructive sleep apnea (OSA) has been proposed as a factor that worsens stroke prognosis. Our aim was to determine if an OSA intervention could improve quality of life (QOL, first objective) and modified Rankin score (mRS, second objective).
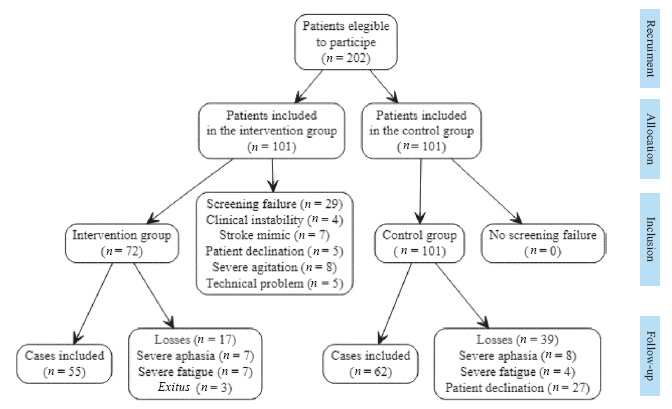
Patients and methods: The intervention group of this quasi-experimental study included patients with acute ischemic stroke <72 hours who underwent polygraphy and Continuous Positive Airway Pressure (CPAP) and hygienic-dietary measures if required. The control group followed routine clinical practice. The Short Form 36 Health Survey (SF-36) and mRS were applied at the sixth month after stroke in both groups.
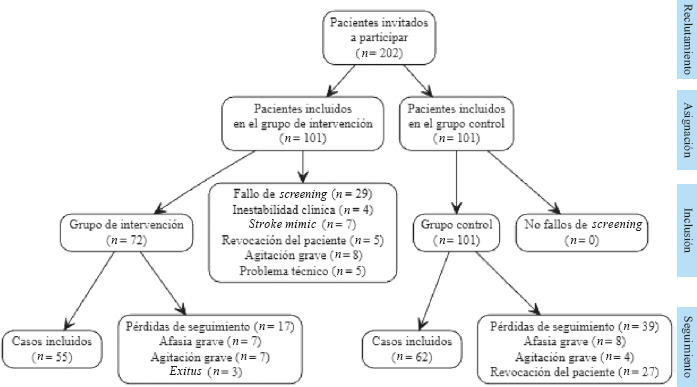
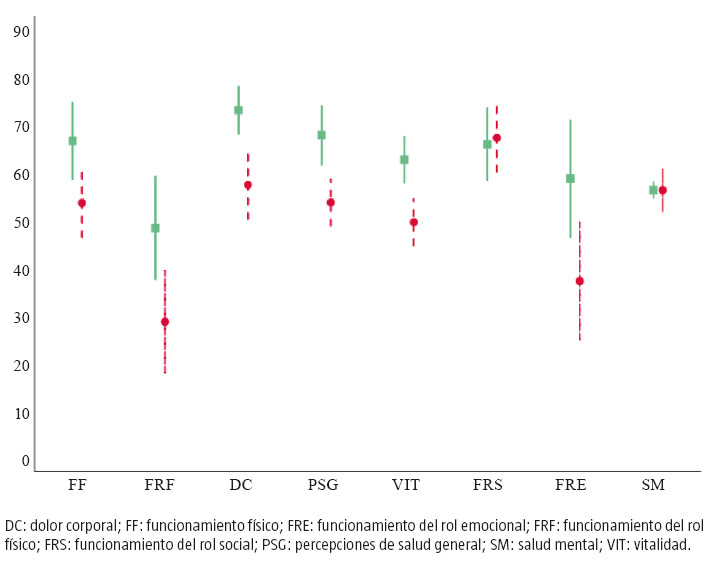
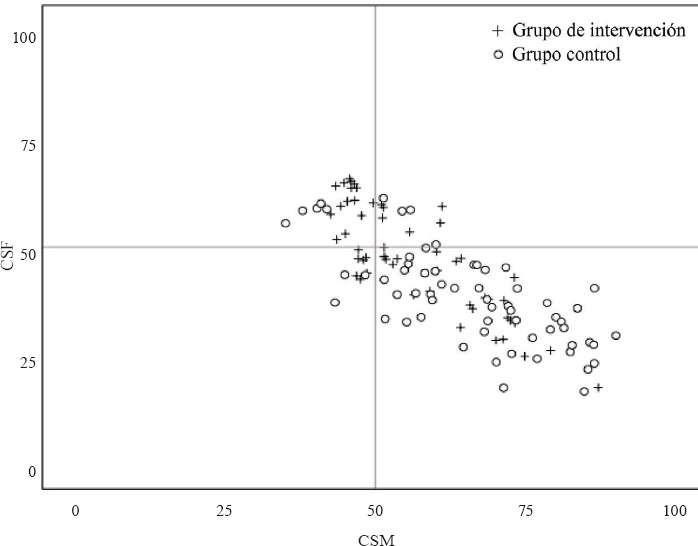
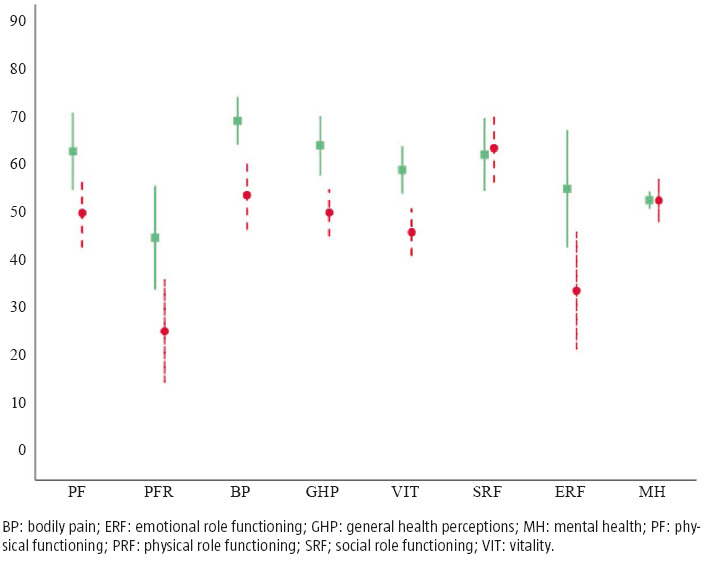
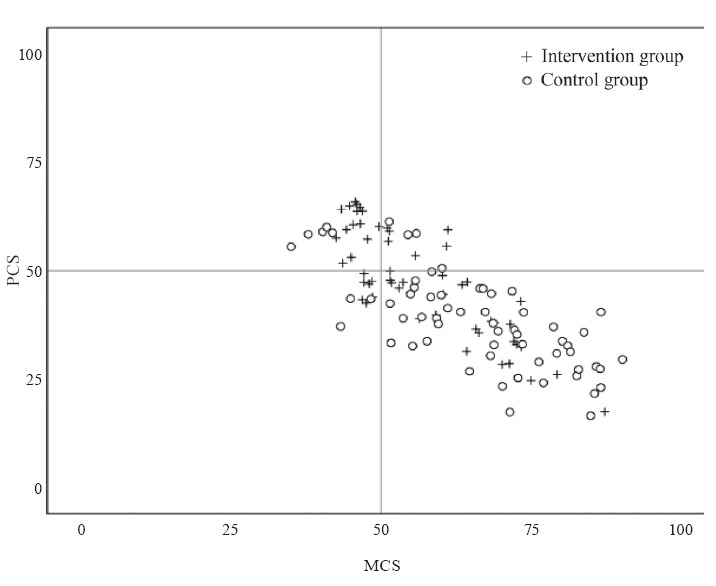
Results: Fifty-five vs. sixty-two patients were included in the intervention and control group respectively. In the intervention group, 64.71% of patients accepted the proposed CPAP (16 cases with a good adherence). An improvement in SF-36 items was detected in the intervention group: physical functioning (p = 0.008), role physical (p = 0.002), bodily pain (p = 0.008), general health (p <0.001), vitality (p = 0.001) and role emotional (p = 0.015). In a per-protocol analysis, all these improvements were verified in the group of patients treated with good CPAP adherence (p < 0.05 in all the same SF-36 items). The percentage of patients with physical component summatory = 50 was higher in the intervention group (p = 0.003). There were no differences in the median of mRS (p = 0.262).
Conclusions: Although more evidence is needed, a significant improvement in QOL was suggested after our OSA intervention, particularly in patients with good CPAP adherence.
Title: Beneficios en la calidad de vida de un programa de cribado y tratamiento de apnea obstructiva del sueño en pacientes con ictus isquémico agudo.
Introducción. La apnea obstructiva del sueño (AOS) se ha propuesto como un factor de mal pronóstico en el ictus. Pretendemos determinar si una intervención sobre la AOS puede mejorar las escalas de calidad de vida (primer objetivo) y de discapacidad (segundo objetivo). Pacientes y métodos. El grupo de intervención de este estudio cuasi experimental incluye a pacientes con ictus isquémico agudo menor de 72 horas de evolución a quienes se les realizó poligrafía, así como presión positiva continua en las vías aéreas (CPAP) y medidas higienicodietéticas si se requerían. En el grupo de control se siguió la práctica clínica habitual. Se aplicaron las escalas Short Form 36 Health Survey (SF-36) y modified Rankin Score (mRS) en el sexto mes del ictus en ambos grupos. Resultados. Se incluyó a 55 y a 62 pacientes en el grupo de intervención y en el de control, respectivamente. En el grupo de intervención, el 64,71% de los pacientes aceptó la CPAP indicada (16 casos con buena adhesión). Se detectó una mejoría en los ítems de la escala SF-36 en el grupo de intervención: funcionamiento físico (p = 0,008), rol físico (p = 0,002), dolor corporal (p = 0,008), salud general (p menor de 0,001), vitalidad (p = 0,001) y rol emocional (p = 0,015). En un análisis por protocolo, todas estas mejorías se comprobaron en el grupo de pacientes tratados con CPAP con buena adhesión (p menor de 0,05 en todos los ítems de la SF-36). El porcentaje de pacientes con el sumatorio del componente físico = 50 fue más alto en el grupo de intervención (p = 0,003). No había diferencias en la mediana de la mRS (p = 0,262). Conclusiones. Aunque se necesitan más evidencias, nuestro estudio sugiere una mejoría significativa de la calidad de vida tras nuestra intervención en la AOS, especialmente en pacientes con buena adhesión a la CPAP.
Conflict of interest statement
Conflicto de intereses: Ninguno.
Figures
References
-
- Sateia MJ. International classification of sleep disorders-third edition highlights and modifications. Chest. 2014;146:1387–94. - PubMed
-
- Loke YK, Brown JWL, Kwok CS, Niruban A, Myint PK. Association of obstructive sleep apnea with risk of serious cardiovascular events:systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2012;5:720–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
