

Machine learning using the extreme gradient boosting (XGBoost) algorithm predicts 5-day delta of SOFA score at ICU admission in COVID-19 patients
- PMID: 36785563
- PMCID: PMC8531027
- DOI: 10.1016/j.jointm.2021.09.002
Machine learning using the extreme gradient boosting (XGBoost) algorithm predicts 5-day delta of SOFA score at ICU admission in COVID-19 patients
Abstract
Background: Accurate risk stratification of critically ill patients with coronavirus disease 2019 (COVID-19) is essential for optimizing resource allocation, delivering targeted interventions, and maximizing patient survival probability. Machine learning (ML) techniques are attracting increased interest for the development of prediction models as they excel in the analysis of complex signals in data-rich environments such as critical care.
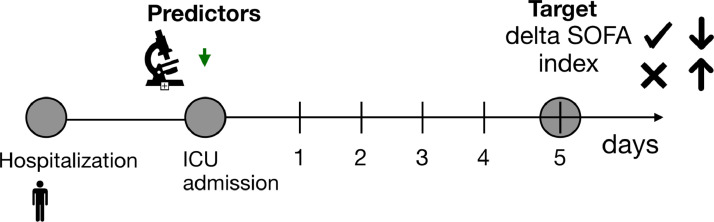
Methods: We retrieved data on patients with COVID-19 admitted to an intensive care unit (ICU) between March and October 2020 from the RIsk Stratification in COVID-19 patients in the Intensive Care Unit (RISC-19-ICU) registry. We applied the Extreme Gradient Boosting (XGBoost) algorithm to the data to predict as a binary outcome the increase or decrease in patients' Sequential Organ Failure Assessment (SOFA) score on day 5 after ICU admission. The model was iteratively cross-validated in different subsets of the study cohort.
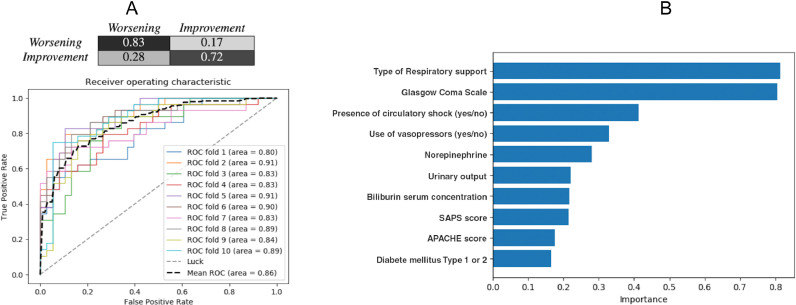
Results: The final study population consisted of 675 patients. The XGBoost model correctly predicted a decrease in SOFA score in 320/385 (83%) critically ill COVID-19 patients, and an increase in the score in 210/290 (72%) patients. The area under the mean receiver operating characteristic curve for XGBoost was significantly higher than that for the logistic regression model (0.86 vs. 0.69, P < 0.01 [paired t-test with 95% confidence interval]).
Conclusions: The XGBoost model predicted the change in SOFA score in critically ill COVID-19 patients admitted to the ICU and can guide clinical decision support systems (CDSSs) aimed at optimizing available resources.
Keywords: COVID-19; Clinical decision support system (CDSS); Extreme gradient boosting (XGBoost); Machine learning; Multiple organ failure; Organ dysfunction score.
© 2021 Chinese Medical Association. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int. [Last accessed on 2021 September 25 ].
LinkOut - more resources
Full Text Sources
