

Comparing SARS-CoV-2 variants among children and adolescents in Germany: relative risk of COVID-19-related hospitalization, ICU admission and mortality
- PMID: 36787015
- PMCID: PMC9925936
- DOI: 10.1007/s15010-023-01996-y
Comparing SARS-CoV-2 variants among children and adolescents in Germany: relative risk of COVID-19-related hospitalization, ICU admission and mortality
Abstract
Purpose: SARS-CoV-2 infections cause COVID-19 and have a wide spectrum of morbidity. Severe disease courses among children are rare. To date, data on the variability of morbidity in relation to variant of concern (VOC) in children has been sparse and inconclusive. We compare the clinical severity of SARS-CoV-2 infection among children and adolescents in Germany during the Wildtype and Alpha combined, Delta and Omicron phases of the COVID-19 pandemic.
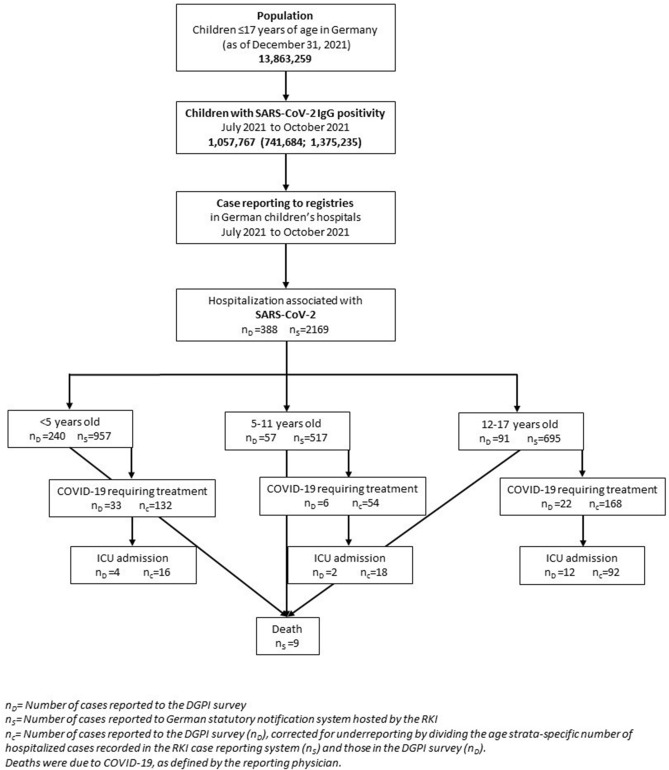
Methods: Comparing risk of COVID-19-related hospitalization, intensive care unit (ICU) admission and death due to COVID-19 in children and adolescents, we used: (1) a multi-center seroprevalence study (SARS-CoV-2-KIDS study); (2) a nationwide registry of pediatric patients hospitalized with SARS-CoV-2 infections; and (3) compulsory national reporting for RT-PCR-confirmed SARS-CoV-2 infections in Germany.
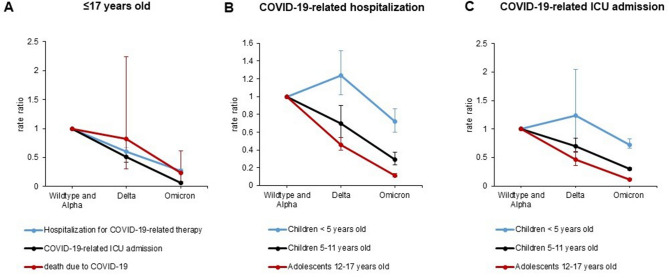
Results: During the Delta predominant phase, risk of COVID-19-related hospitalization among all SARS-CoV-2 seropositive children was 3.35, ICU admission 1.19 and fatality 0.09 per 10,000; hence about halved for hospitalization and ICU admission and unchanged for deaths as compared to the Wildtype- and Alpha-dominant period. The relative risk for COVID-19-related hospitalization and ICU admission compared to the alpha period decreased during Delta [0.60 (95% CI 0.54; 0.67) and 0.51 (95% CI 0.42; 0.61)] and Omicron [0.27 (95% CI 0.24; 0.30) and 0.06 (95% CI 0.05; 0.08)] period except for the < 5-year-olds. The rate of case fatalities decreased slightly during Delta, and substantially during Omicron phase.
Conclusion: Morbidity caused by SARS-CoV-2 infections among children and adolescents in Germany decreased over the course of the COVID-19 pandemic, as different VOCs) emerged.
Keywords: Adolescents; Burden of disease; COVID-19; Children; Pandemic; SARS-CoV-2; Seroprevalence; Variants of concern.
© 2023. The Author(s).
Conflict of interest statement
The participating pediatric hospitals received academic research funding from the Federal Ministry of Education and Research (BMBF) for study planning, study management and reimbursement for the assay of this study. No other relevant financial or non-financial conflicts were reported.
Figures
References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
