

Assessment of Symptom, Disability, and Financial Trajectories in Patients Hospitalized for COVID-19 at 6 Months
- PMID: 36787143
- PMCID: PMC9929698
- DOI: 10.1001/jamanetworkopen.2022.55795
Assessment of Symptom, Disability, and Financial Trajectories in Patients Hospitalized for COVID-19 at 6 Months
Abstract
Importance: Individuals who survived COVID-19 often report persistent symptoms, disabilities, and financial consequences. However, national longitudinal estimates of symptom burden remain limited.
Objective: To measure the incidence and changes over time in symptoms, disability, and financial status after COVID-19-related hospitalization.
Design, setting, and participants: A national US multicenter prospective cohort study with 1-, 3-, and 6-month postdischarge visits was conducted at 44 sites participating in the National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Network's Biology and Longitudinal Epidemiology: COVID-19 Observational (BLUE CORAL) study. Participants included hospitalized English- or Spanish-speaking adults without severe prehospitalization disabilities or cognitive impairment. Participants were enrolled between August 24, 2020, and July 20, 2021, with follow-up occurring through March 30, 2022.
Exposure: Hospitalization for COVID-19 as identified with a positive SARS-CoV-2 molecular test.
Main outcomes and measures: New or worsened cardiopulmonary symptoms, financial problems, functional impairments, perceived return to baseline health, and quality of life. Logistic regression was used to identify factors associated with new cardiopulmonary symptoms or financial problems at 6 months.
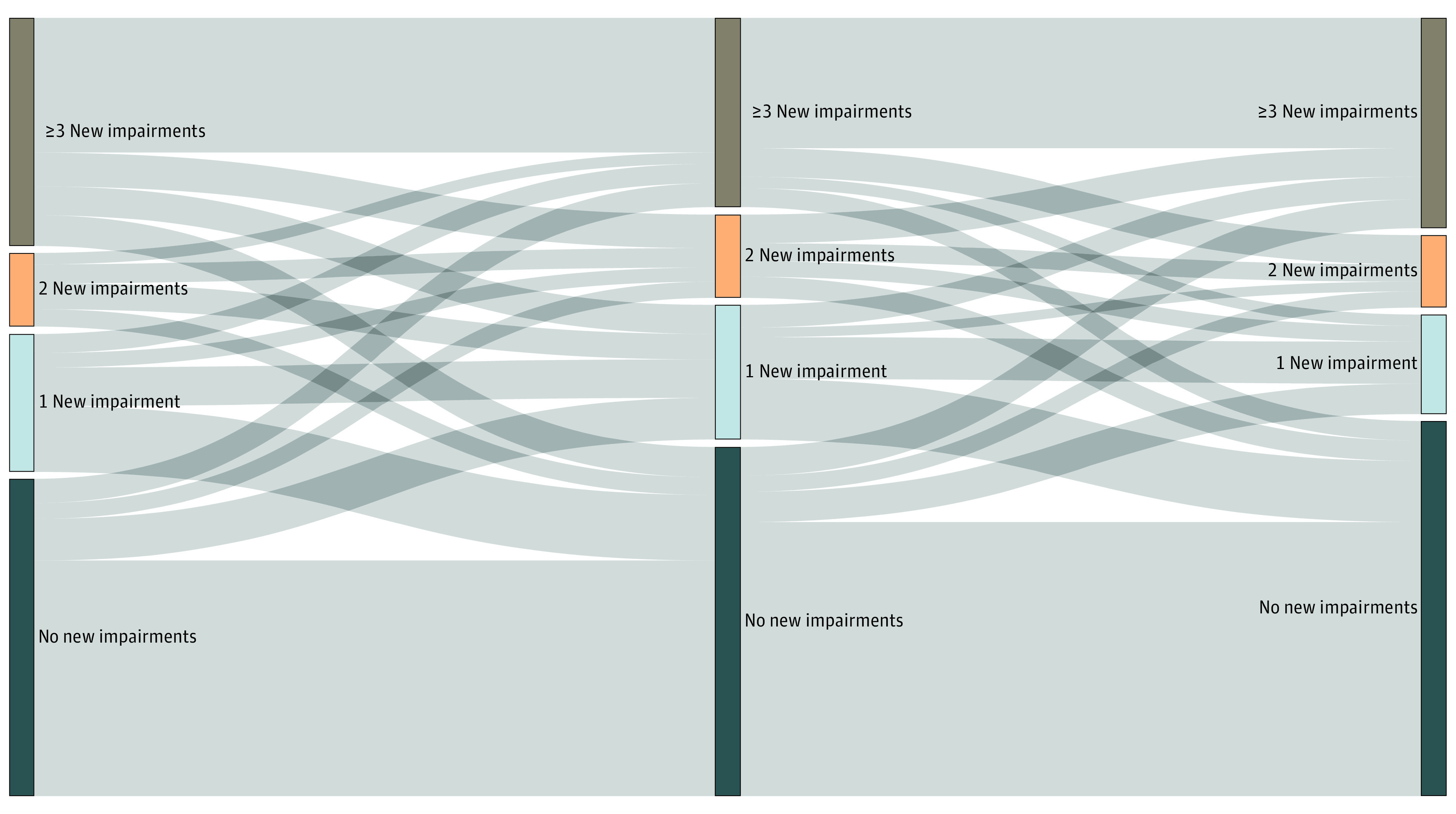
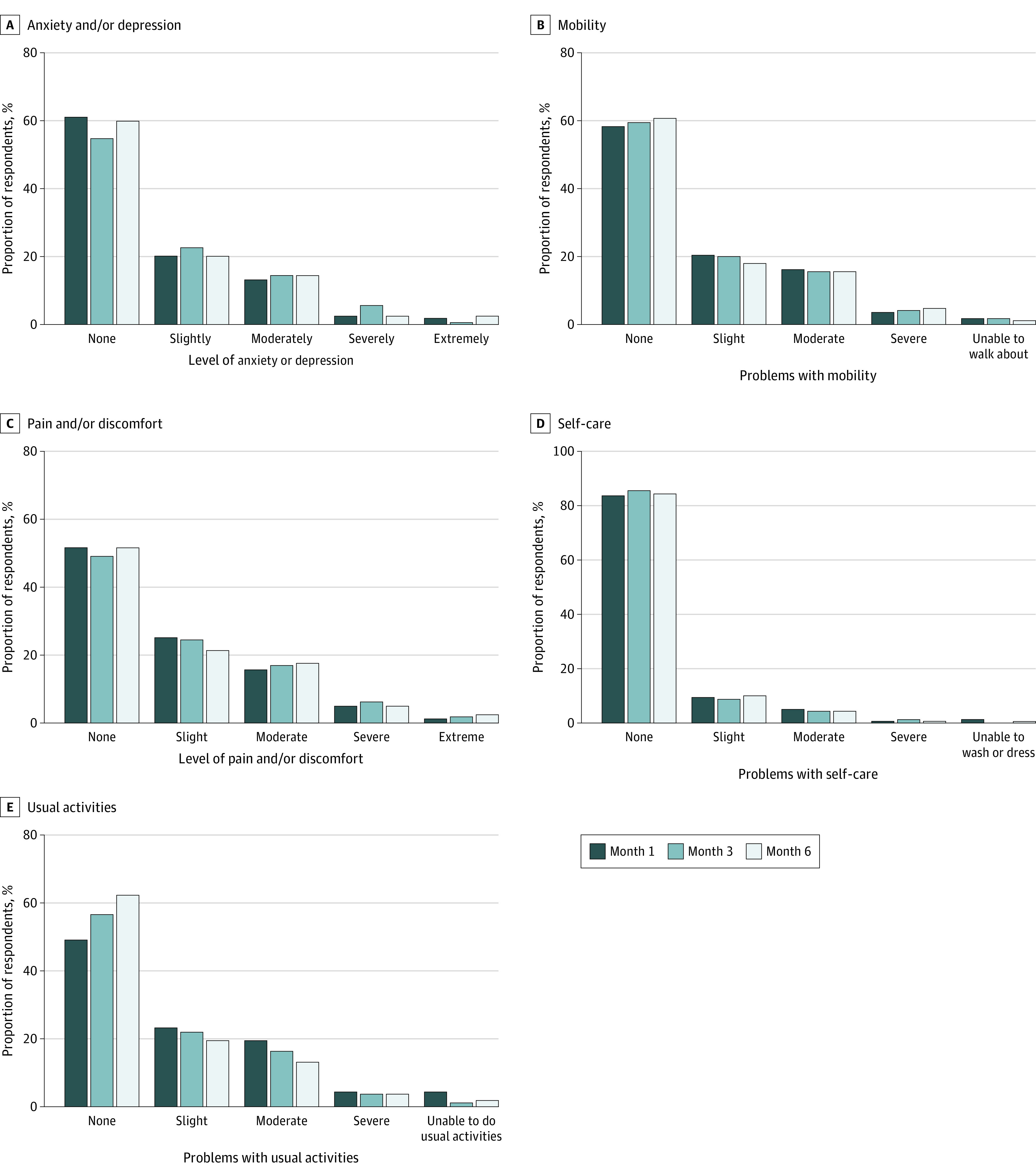
Results: A total of 825 adults (444 [54.0%] were male, and 379 [46.0%] were female) met eligibility criteria and completed at least 1 follow-up survey. Median age was 56 (IQR, 43-66) years; 253 (30.7%) participants were Hispanic, 145 (17.6%) were non-Hispanic Black, and 360 (43.6%) were non-Hispanic White. Symptoms, disabilities, and financial problems remained highly prevalent among hospitalization survivors at month 6. Rates increased between months 1 and 6 for cardiopulmonary symptoms (from 67.3% to 75.4%; P = .001) and fatigue (from 40.7% to 50.8%; P < .001). Decreases were noted over the same interval for prevalent financial problems (from 66.1% to 56.4%; P < .001) and functional limitations (from 55.3% to 47.3%; P = .004). Participants not reporting problems at month 1 often reported new symptoms (60.0%), financial problems (23.7%), disabilities (23.8%), or fatigue (41.4%) at month 6.
Conclusions and relevance: The findings of this cohort study of people discharged after COVID-19 hospitalization suggest that recovery in symptoms, functional status, and fatigue was limited at 6 months, and some participants reported new problems 6 months after hospital discharge.
Conflict of interest statement
Figures
References
-
- Evans RA, McAuley H, Harrison EM, et al. ; PHOSP-COVID Collaborative Group . Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): a UK multicentre, prospective cohort study. Lancet Respir Med. 2021;9(11):1275-1287. doi: 10.1016/S2213-2600(21)00383-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL123010/HL/NHLBI NIH HHS/United States
- K08 HL155407/HL/NHLBI NIH HHS/United States
- T32 HD007339/HD/NICHD NIH HHS/United States
- U01 HL123009/HL/NHLBI NIH HHS/United States
- K01 HL140279/HL/NHLBI NIH HHS/United States
- U01 HL123023/HL/NHLBI NIH HHS/United States
- U01 HL122989/HL/NHLBI NIH HHS/United States
- U01 HL123008/HL/NHLBI NIH HHS/United States
- U01 HL123027/HL/NHLBI NIH HHS/United States
- U01 HL123033/HL/NHLBI NIH HHS/United States
- U01 HL123022/HL/NHLBI NIH HHS/United States
- R01 HL155064/HL/NHLBI NIH HHS/United States
- U01 HL123004/HL/NHLBI NIH HHS/United States
- U01 HL122998/HL/NHLBI NIH HHS/United States
- U01 HL123031/HL/NHLBI NIH HHS/United States
- U01 HL123020/HL/NHLBI NIH HHS/United States
- K08 HL148514/HL/NHLBI NIH HHS/United States
- K23 AR079583/AR/NIAMS NIH HHS/United States
- U01 HL123018/HL/NHLBI NIH HHS/United States
- L32 MD017732/MD/NIMHD NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- IK2 HX003005/HX/HSRD VA/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
