

CD70 is a therapeutic target upregulated in EMT-associated EGFR tyrosine kinase inhibitor resistance
- PMID: 36787696
- PMCID: PMC10259078
- DOI: 10.1016/j.ccell.2023.01.007
CD70 is a therapeutic target upregulated in EMT-associated EGFR tyrosine kinase inhibitor resistance
Abstract
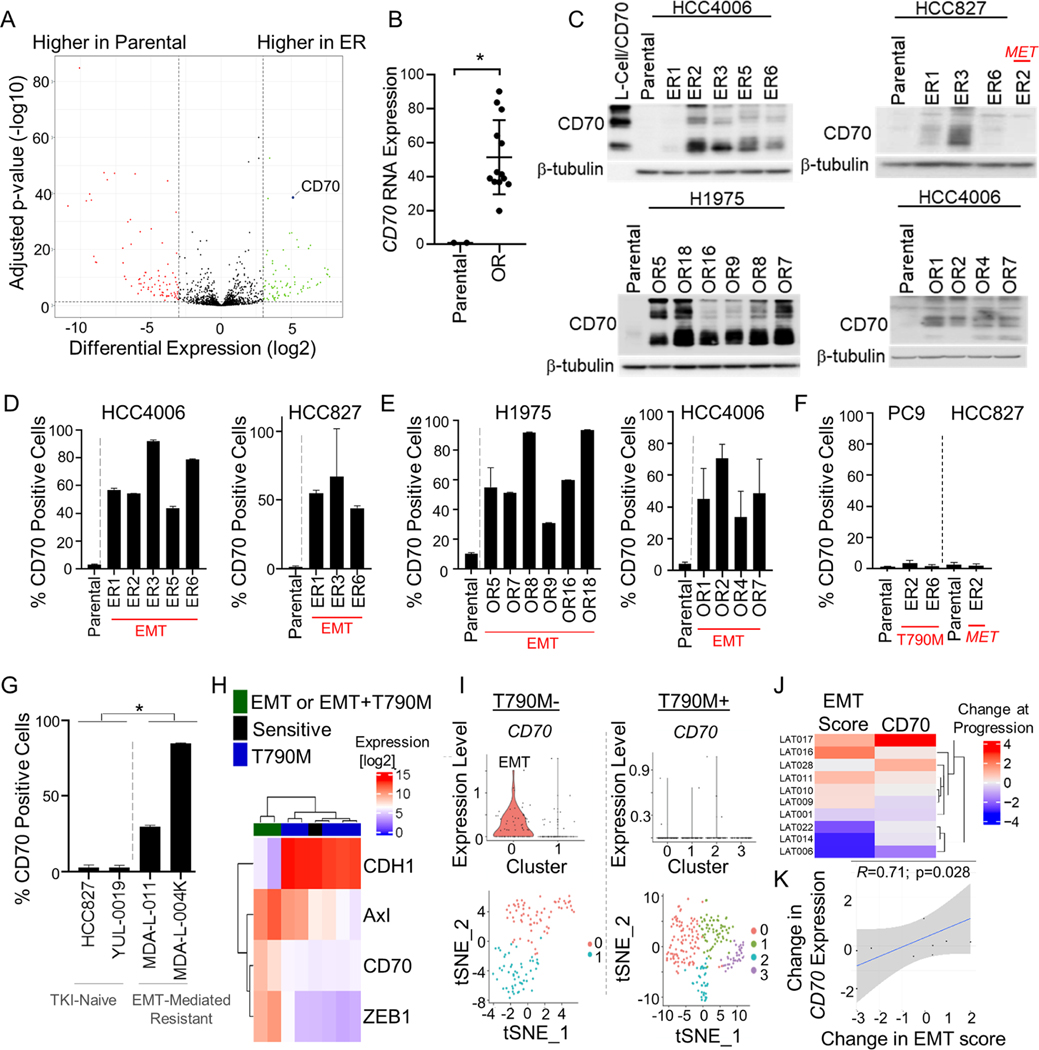
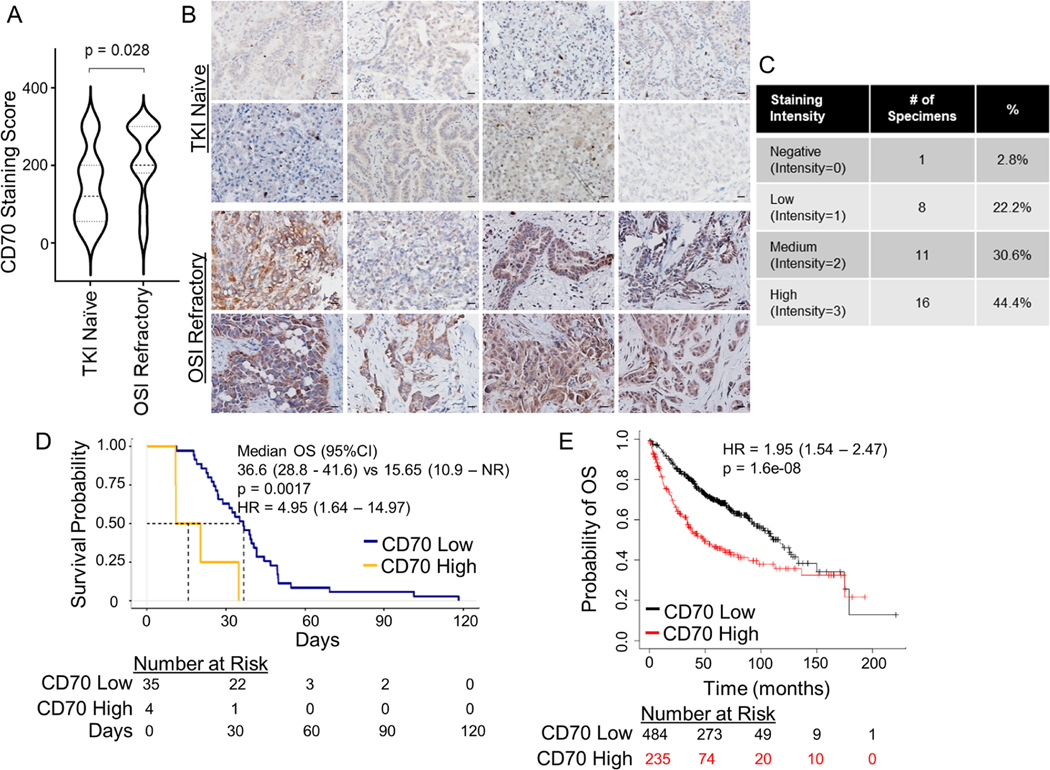
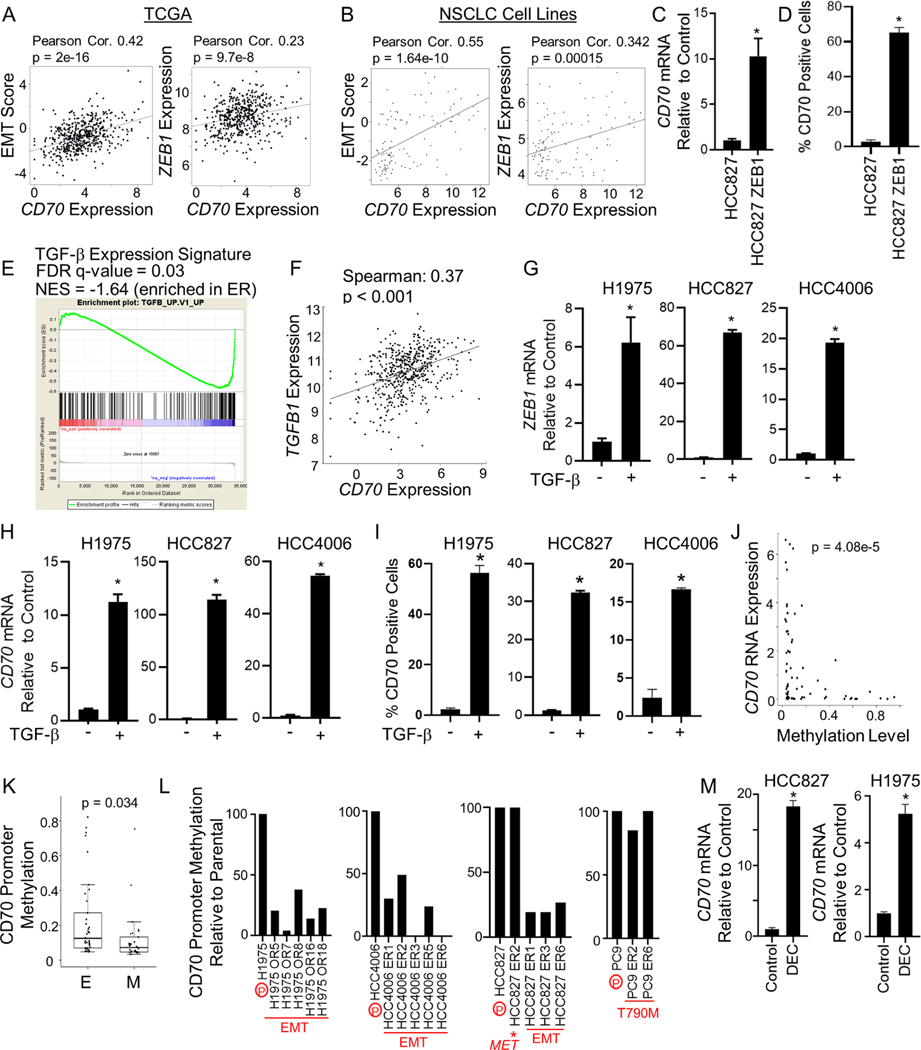
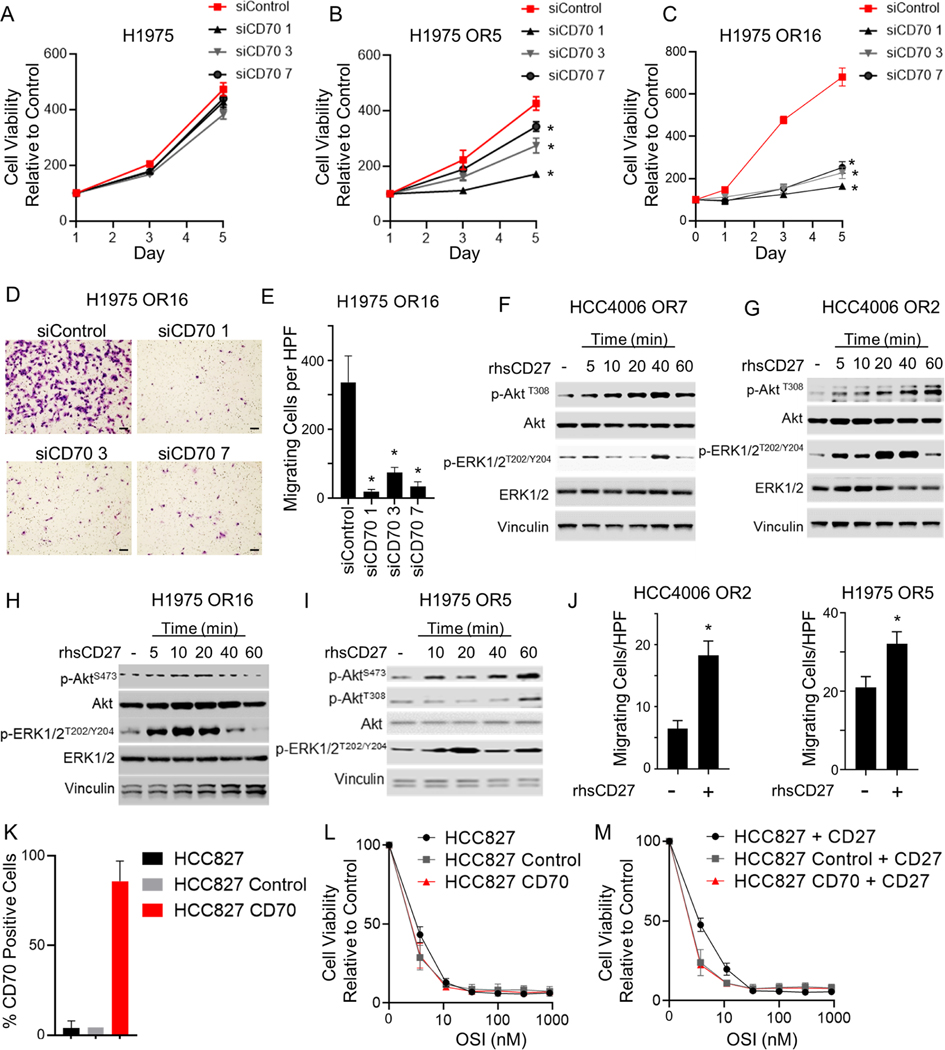
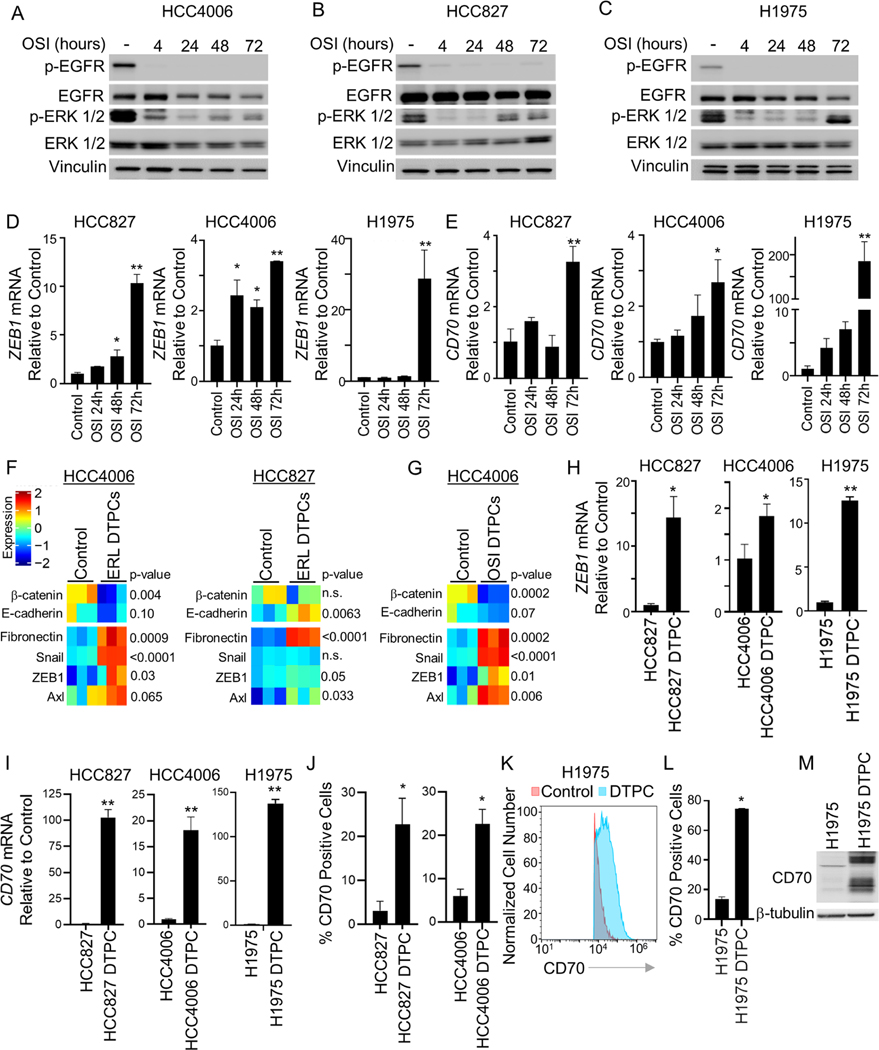
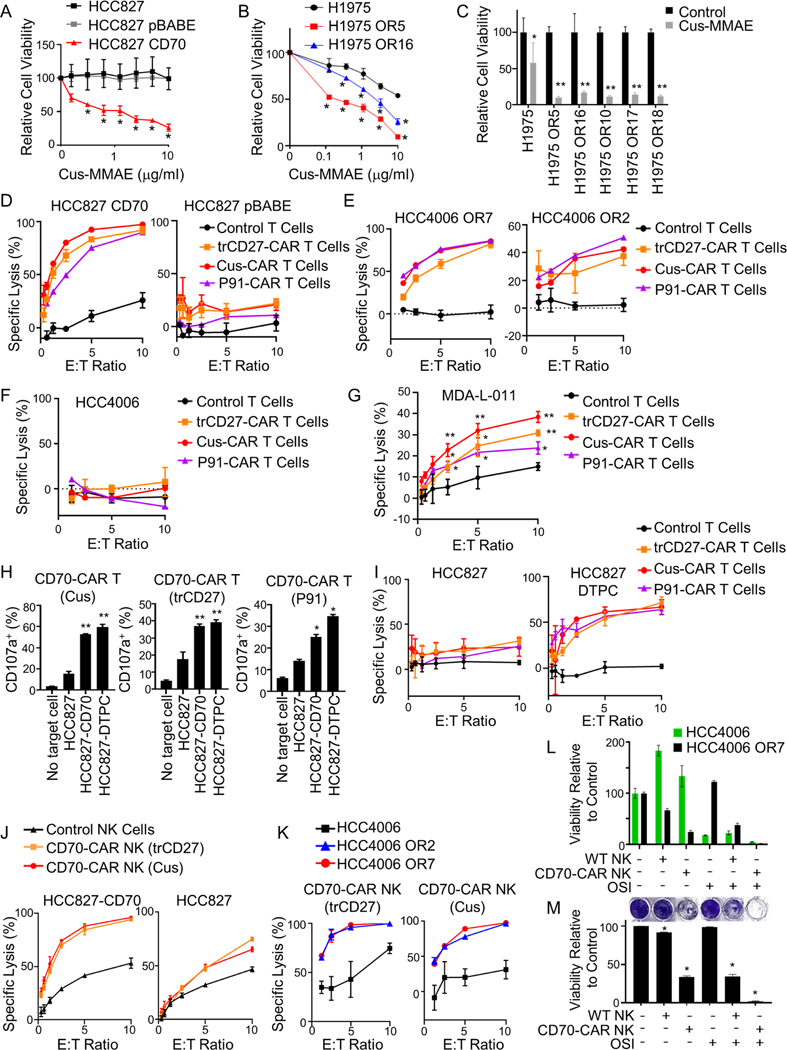
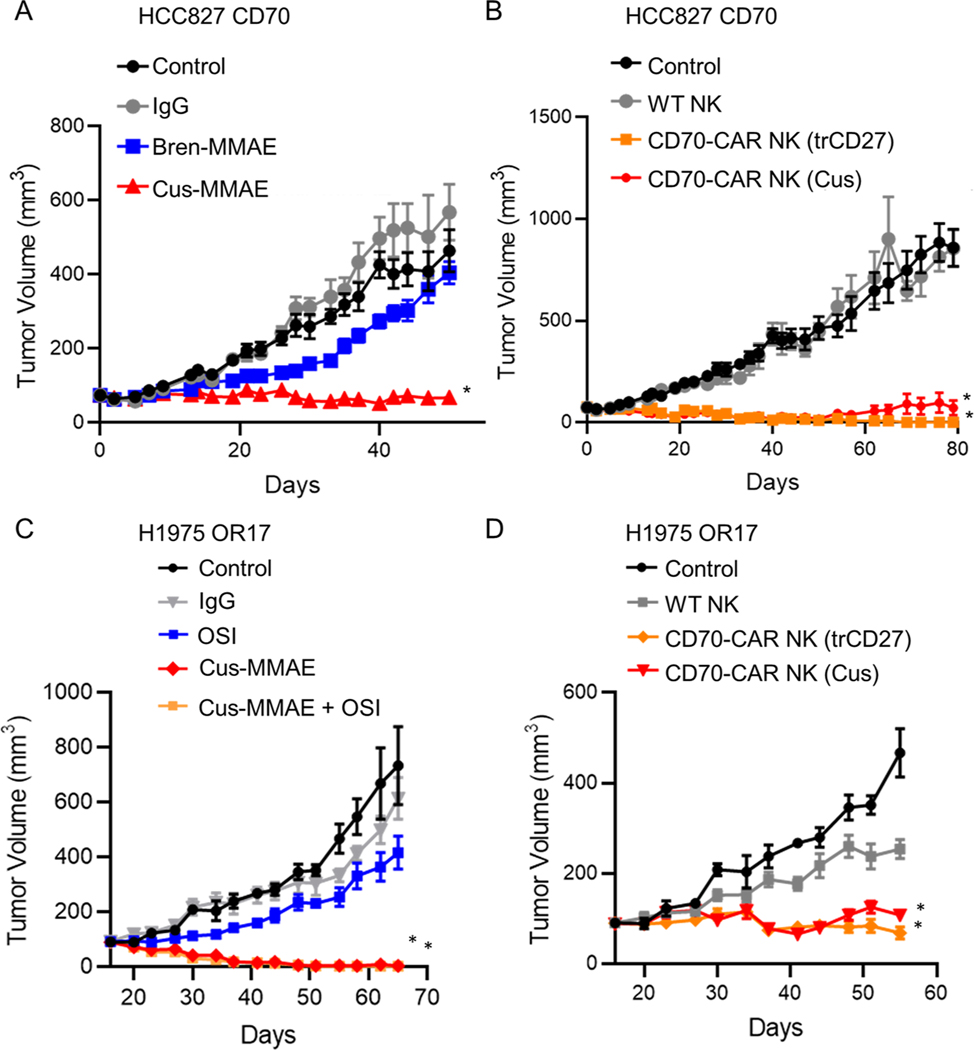
Effective therapeutic strategies are needed for non-small cell lung cancer (NSCLC) patients with epidermal growth factor receptor (EGFR) mutations that acquire resistance to EGFR tyrosine kinase inhibitors (TKIs) mediated by epithelial-to-mesenchymal transition (EMT). We investigate cell surface proteins that could be targeted by antibody-based or adoptive cell therapy approaches and identify CD70 as being highly upregulated in EMT-associated resistance. Moreover, CD70 upregulation is an early event in the evolution of resistance and occurs in drug-tolerant persister cells (DTPCs). CD70 promotes cell survival and invasiveness, and stimulation of CD70 triggers signal transduction pathways known to be re-activated with acquired TKI resistance. Anti-CD70 antibody drug conjugates (ADCs) and CD70-targeting chimeric antigen receptor (CAR) T cell and CAR NK cells show potent activity against EGFR TKI-resistant cells and DTPCs. These results identify CD70 as a therapeutic target for EGFR mutant tumors with acquired EGFR TKI resistance that merits clinical investigation.
Keywords: CD70; EGFR; NSCLC.
Copyright © 2023. Published by Elsevier Inc.
Conflict of interest statement
Declaration of interests J.V.H. serves on advisory committees for DAVA Oncology, Regeneron, BerGenBio, Jazz Pharmaceuticals, Curio Science, Immunocore, AstraZeneca, EMD Serono, Boehringer-Ingelheim, Catalyst, Genentech, GlaxoSmithKline, Guardant Health, Foundation Medicine, Hengrui Therapeutics, Eli Lilly, Novartis, Spectrum, Sanofi, Takeda, Mirati Therapeutics, BMS, BrightPath Biotherapeutics, Janssen Global Services, Nexus Health Systems, Pneuma Respiratory, Kairos Venture Investments, Roche, Leads Biolabs, RefleXion, and Chugai Pharmaceuticals; receives research support from Takeda, AstraZeneca, Boehringer-Ingelheim, and Spectrum; and receives royalties and licensing fees from Spectrum Pharmaceuticals. D.L.G. serves as an advisor/consultant for Sanofi, GlaxoSmithKline, Janssen Research & Development, Ribon Therapeutics, Mitobridge, Eli Lilly, Menarini, and Napa Therapeutics and receives research funding from Janssen Research & Development, Takeda, AstraZeneca, Mitobridge, Ribon Therapeutics, NGM Biopharmaceuticals, Boehringer Ingelheim, and Mirati Therapeutics. S.S.K. reports research support from Boehringer Ingelheim, Janssen, MiNA Therapeutics, MiRXES, and Taiho Therapeutics and honoraria from Boehringer Ingelheim, Bristol Meyers Squibb, AstraZeneca, Chugai Pharmaceutical, and Takeda Pharmaceuticals, all outside of the submitted work. X.L. receives consulting/advisory fees from EMD Serono (Merck KGaA), AstraZeneca, Spectrum Pharmaceutics, Novartis, Eli Lilly, Boehringer Ingelheim, Hengrui Therapeutics, Janssen, Blueprint Medicines, Sensei Biotherapeutics, and AbbVie and received research funding from Eli Lilly, EMD Serono, Regeneron, and Boehringer Ingelheim. M.B.N. and J.P.R. receive royalties and licensing fees from Spectrum Pharmaceuticals. M.B.N. and J.V.H. have filed a patent for CD70 targeting in EGFR TKI-resistant NSCLC (17/611,019). J.P.R. is currently a full-time employee and shareholder of AstraZeneca. Y.Y.E. discloses research support from AstraZeneca, Takeda, Eli Lilly, Xcovery, Tuning Point Therapeutics, BluPrint, and Elevation Oncology; an advisory role for AstraZeneca, Eli Lilly, Takeda, Spectrum, Bristol Myers Squibb, and Turning Point; and accommodation expenses from Eli Lilly. H.U. receives research support from Takeda Pharmaceuticals and Boehringer Ingelheim. S.H. receives consulting fees from AstraZeneca and Boehringer Ingelheim and speaker fees from Qiagen.
Figures
References
-
- Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, et al. (2012). Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. The Lancet. Oncology 13, 239–246. 10.1016/S1470-2045(11)70393-X. - DOI - PubMed
-
- Sequist LV., Martins RG., Spigel D., Grunberg SM., Spira A., Janne PA., Joshi VA., McCollum D., Evans TL., Muzikansky A., et al. (2008). First-line gefitinib in patients with advanced non-small-cell lung cancer harboring somatic EGFR mutations. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 26, 2442–2449. 10.1200/JCO.2007.14.8494. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
