

Machine learning determination of motivators of terminal extubation during the transition to end-of-life care in intensive care unit
- PMID: 36788319
- PMCID: PMC9929077
- DOI: 10.1038/s41598-023-29042-9
Machine learning determination of motivators of terminal extubation during the transition to end-of-life care in intensive care unit
Abstract
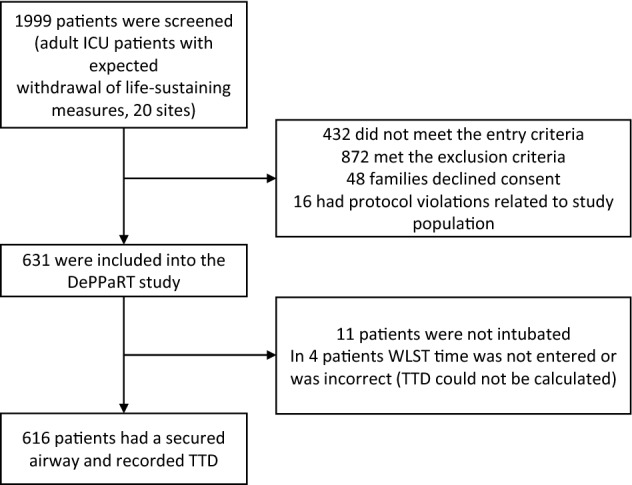
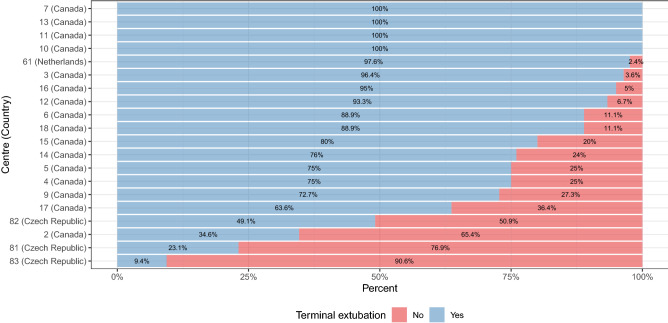
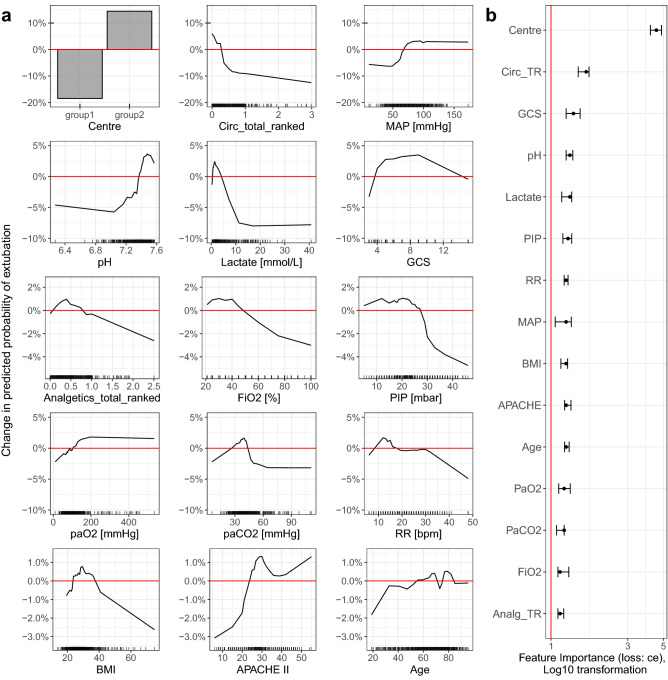
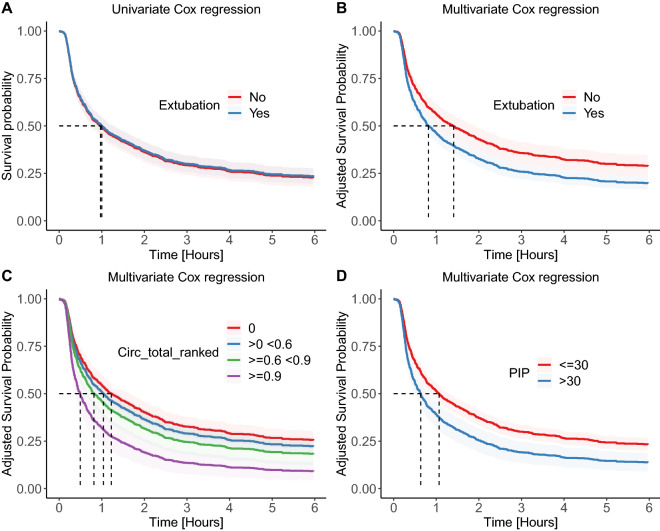
Procedural aspects of compassionate care such as the terminal extubation are understudied. We used machine learning methods to determine factors associated with the decision to extubate the critically ill patient at the end of life, and whether the terminal extubation shortens the dying process. We performed a secondary data analysis of a large, prospective, multicentre, cohort study, death prediction and physiology after removal of therapy (DePPaRT), which collected baseline data as well as ECG, pulse oximeter and arterial waveforms from WLST until 30 min after death. We analysed a priori defined factors associated with the decision to perform terminal extubation in WLST using the random forest method and logistic regression. Cox regression was used to analyse the effect of terminal extubation on time from WLST to death. A total of 616 patients were included into the analysis, out of which 396 (64.3%) were terminally extubated. The study centre, low or no vasopressor support, and good respiratory function were factors significantly associated with the decision to extubate. Unadjusted time to death did not differ between patients with and without extubation (median survival time extubated vs. not extubated: 60 [95% CI: 46; 76] vs. 58 [95% CI: 45; 75] min). In contrast, after adjustment for confounders, time to death of extubated patients was significantly shorter (49 [95% CI: 40; 62] vs. 85 [95% CI: 61; 115] min). The decision to terminally extubate is associated with specific centres and less respiratory and/or vasopressor support. In this context, terminal extubation was associated with a shorter time to death.
© 2023. The Author(s).
Conflict of interest statement
Dr. Scales, Dr. van Beinum, Ms. Hornby and Dr. Dhanani are named on a patent related to estimating the time to death employing variability monitoring and physiological waveform analysis (System and method for assisting decisions associated with events relative to withdrawal of life-sustaining therapy using variability measurements AJE Seely, S Dhanani, B Nathan, CL Herry, L Hornby, TO Ramsay, US Patent 10,172,569). Ms. Hornby is paid research consultant for the Canadian Blood Services Dr. Dhanani and Dr. Shemie are medical advisors for deceased donation with Canadian Blood Services. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Similar articles
-
Daytime Versus Nighttime Extubations: A Comparison of Reintubation, Length of Stay, and Mortality.J Intensive Care Med. 2016 Feb;31(2):118-26. doi: 10.1177/0885066614531392. Epub 2014 Apr 24. J Intensive Care Med. 2016. PMID: 24763118
-
Ventilator Weaning and Terminal Extubation: Withdrawal of Life-Sustaining Therapy in Children. Secondary Analysis of the Death One Hour After Terminal Extubation Study.Crit Care Med. 2024 Mar 1;52(3):396-406. doi: 10.1097/CCM.0000000000006101. Epub 2023 Oct 27. Crit Care Med. 2024. PMID: 37889228 Free PMC article.
-
Terminal weaning or immediate extubation for withdrawing mechanical ventilation in critically ill patients (the ARREVE observational study).Intensive Care Med. 2017 Dec;43(12):1793-1807. doi: 10.1007/s00134-017-4891-0. Epub 2017 Sep 22. Intensive Care Med. 2017. PMID: 28936597
-
Weaning from the ventilator and extubation in ICU.Curr Opin Crit Care. 2013 Feb;19(1):57-64. doi: 10.1097/MCC.0b013e32835c5095. Curr Opin Crit Care. 2013. PMID: 23235542 Review.
-
Who Is Safe to Extubate in the Neuroscience Intensive Care Unit?Semin Respir Crit Care Med. 2017 Dec;38(6):830-839. doi: 10.1055/s-0037-1608773. Epub 2017 Dec 20. Semin Respir Crit Care Med. 2017. PMID: 29262440 Review.
Cited by
-
Intensive care clinicians' experiences of palliative withdrawal of mechanical ventilation: a qualitative study.BMJ Open. 2025 Aug 8;15(8):e096527. doi: 10.1136/bmjopen-2024-096527. BMJ Open. 2025. PMID: 40780709 Free PMC article.
-
Organ donation after death determination by circulatory criteria: family members' experiences with withdrawal of life-sustaining measures in Canadian intensive care units.Can J Anaesth. 2025 Jun;72(6):975-985. doi: 10.1007/s12630-025-02978-4. Epub 2025 Jun 26. Can J Anaesth. 2025. PMID: 40571891 English.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
