

Evaluation of muco-adhesive tacrolimus patch on caspase-3 induced apoptosis in oral lichen planus: a randomized clinical trial
- PMID: 36788511
- PMCID: PMC9930326
- DOI: 10.1186/s12903-023-02803-8
Evaluation of muco-adhesive tacrolimus patch on caspase-3 induced apoptosis in oral lichen planus: a randomized clinical trial
Abstract
Background: The study compared the clinical effectiveness of topical Tacrolimus (TAC) in patches or gel with Triamcinolone acetonide (TRI) gel for erosive/atrophic oral lichen planus (OLP) and investigated the influence of these therapies on Caspase-3 expression as a marker of apoptosis.
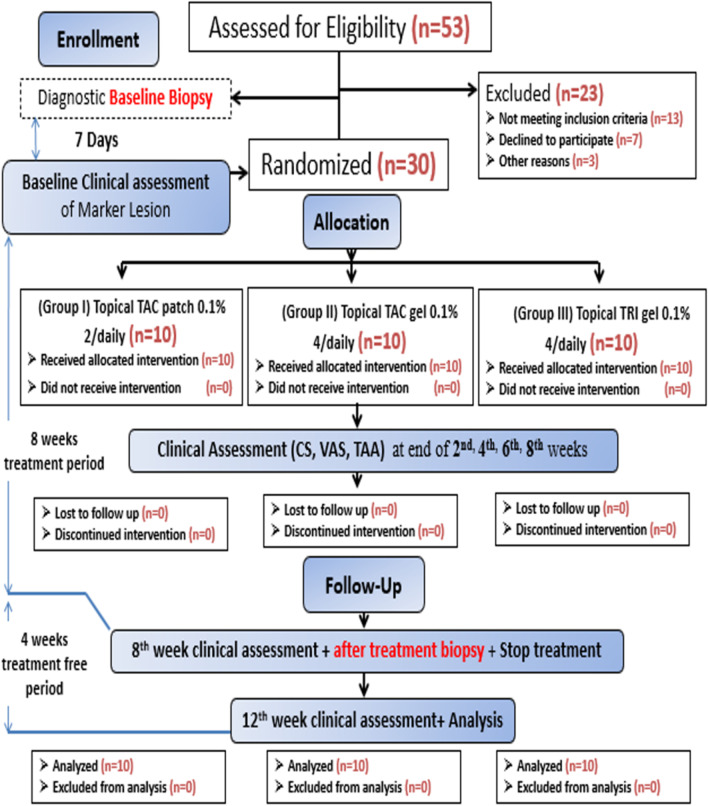
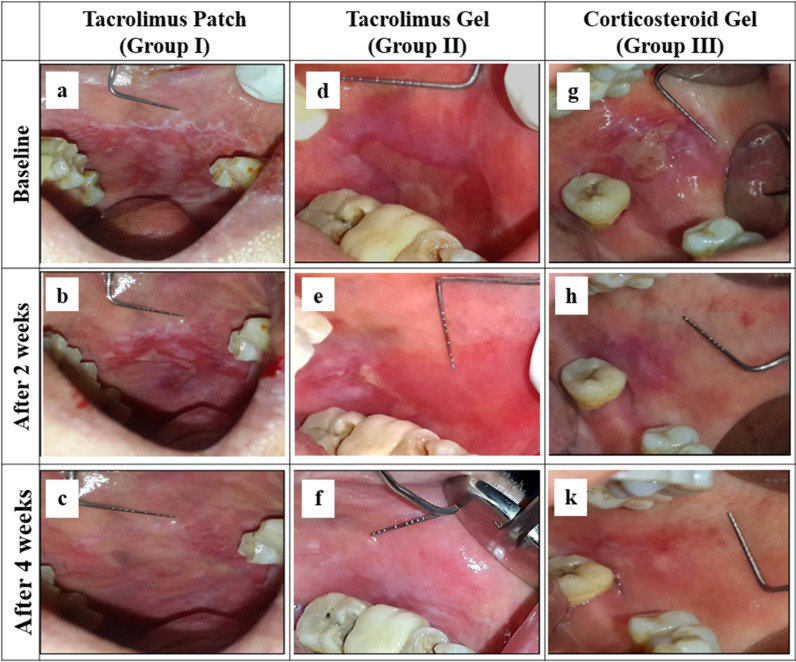
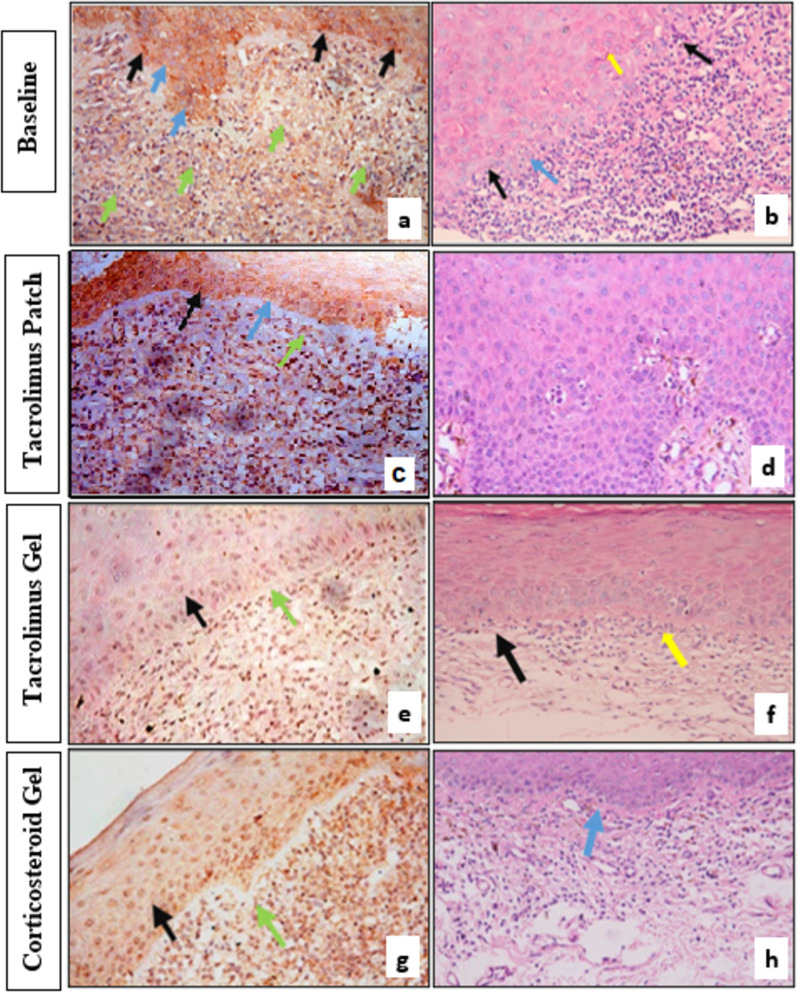
Methods: Thirty patients were randomly assigned into three equal groups to receive either topical TAC 0.1% patch twice daily, topical TAC 0.1% gel, or topical TRI 0.1% gel four times daily for 8 weeks. Each patient's clinical score (CS), visual analogue scale (VAS), and total atrophic area (TAA) of the marker lesion were measured at baseline, 2, 4, and 8 weeks of treatment, as well as after 4 weeks of treatment free period. Caspase-3 expression and lymphocytic counts (LC) were assessed in pre- and post-treatment biopsied stained sections.
Results: TAC patch resulted in a higher reduction in CS [- 14.00 (15.54%)] and VAS [- 70.21 (15.82%)] followed by TAC gel then TRI gel within the first two weeks. The reduction in VAS and TAA were significantly higher in TAC groups compared to TRI gel, although the difference between TAC treatment was not significant and this was observed throughout the treatment and follow-up periods. Caspase-3 expression increased in connective tissue in all groups. It decreased significantly within the epithelium in both TAC groups but increased in TRI gel. (LC) were significantly lowered with the TAC patch compared to other groups. The percentage change in Caspase-3 epithelial expression was significantly correlated to the CS, TAA, and LC.
Conclusion: Both TAC patch and gel significantly decreased pain and lesion size than TRI gel, with a significant reduction in Caspase-3 expression within the epithelium in comparison to the increase seen with TRI gel. The study protocol was registered at www.
Clinicaltrials: gov (NCT05139667) on 01/12/2021.
Keywords: Apoptotic keratinocytes; Caspase-3; Oral lichen planus; Tacrolimus; Triamcinolone acetonide.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
