

CRISIS AFAR: an international collaborative study of the impact of the COVID-19 pandemic on mental health and service access in youth with autism and neurodevelopmental conditions
- PMID: 36788583
- PMCID: PMC9928142
- DOI: 10.1186/s13229-022-00536-z
CRISIS AFAR: an international collaborative study of the impact of the COVID-19 pandemic on mental health and service access in youth with autism and neurodevelopmental conditions
Abstract
Background: Heterogeneous mental health outcomes during the COVID-19 pandemic are documented in the general population. Such heterogeneity has not been systematically assessed in youth with autism spectrum disorder (ASD) and related neurodevelopmental disorders (NDD). To identify distinct patterns of the pandemic impact and their predictors in ASD/NDD youth, we focused on pandemic-related changes in symptoms and access to services.
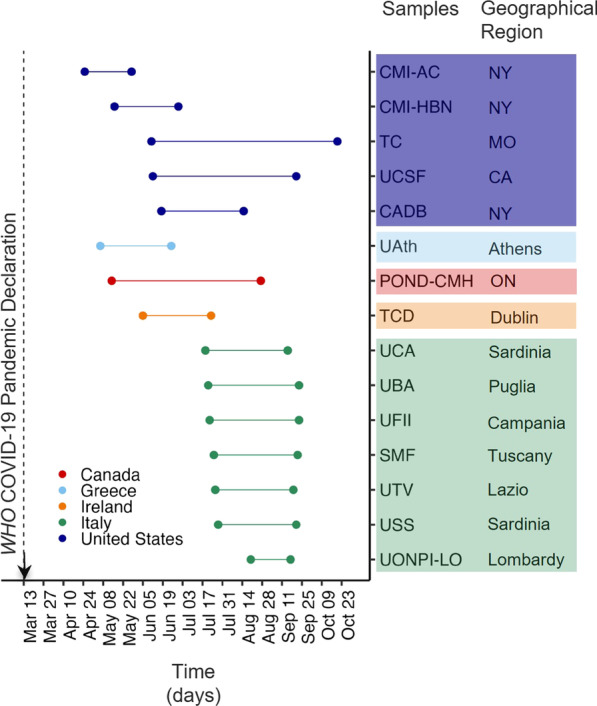
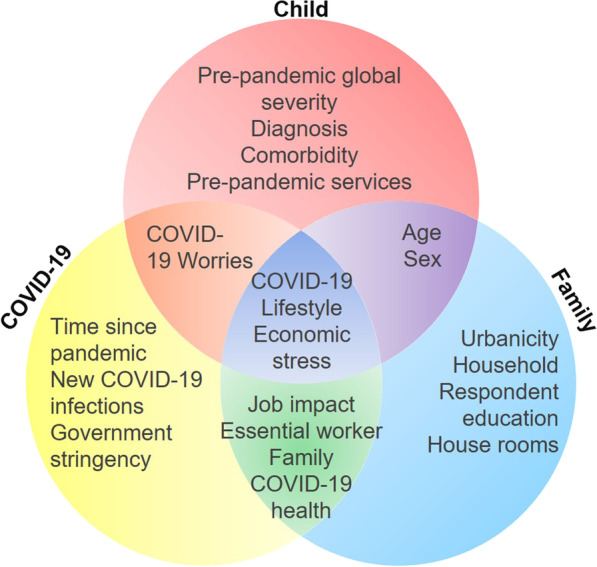
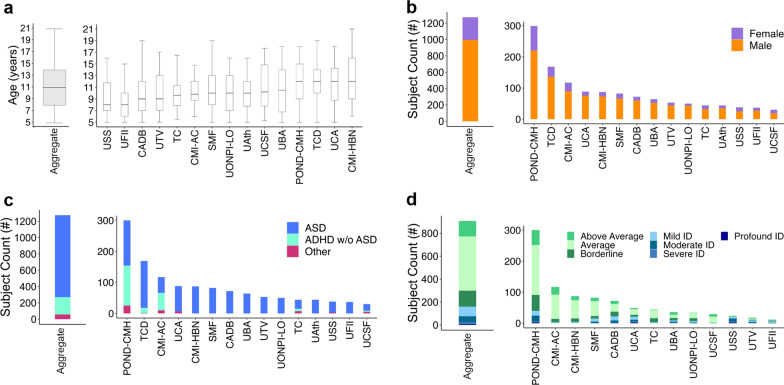
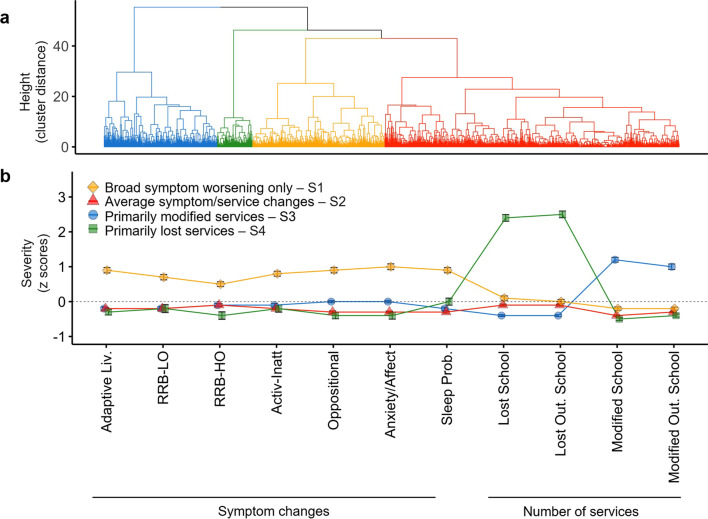
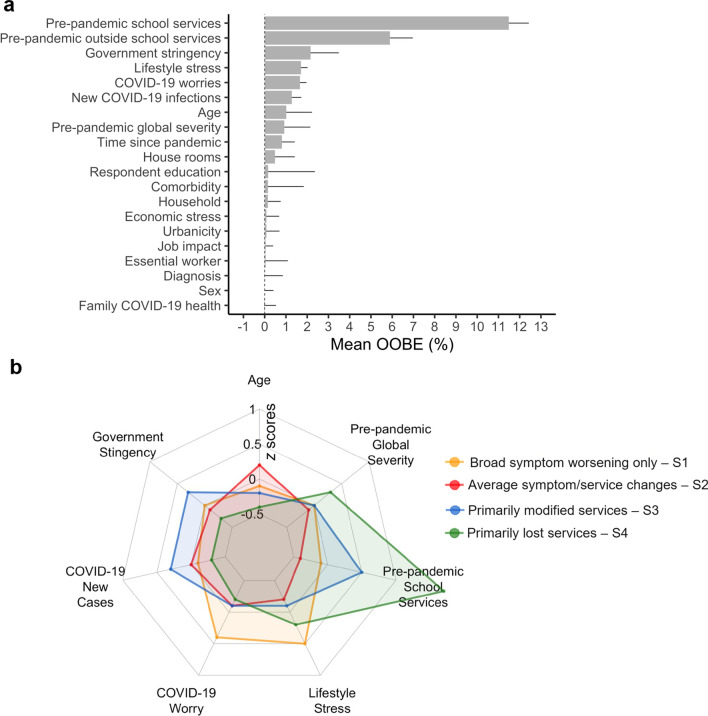
Methods: Using a naturalistic observational design, we assessed parent responses on the Coronavirus Health and Impact Survey Initiative (CRISIS) Adapted For Autism and Related neurodevelopmental conditions (AFAR). Cross-sectional AFAR data were aggregated across 14 European and North American sites yielding a clinically well-characterized sample of N = 1275 individuals with ASD/NDD (age = 11.0 ± 3.6 years; n females = 277). To identify subgroups with differential outcomes, we applied hierarchical clustering across eleven variables measuring changes in symptoms and access to services. Then, random forest classification assessed the importance of socio-demographics, pre-pandemic service rates, clinical severity of ASD-associated symptoms, and COVID-19 pandemic experiences/environments in predicting the outcome subgroups.
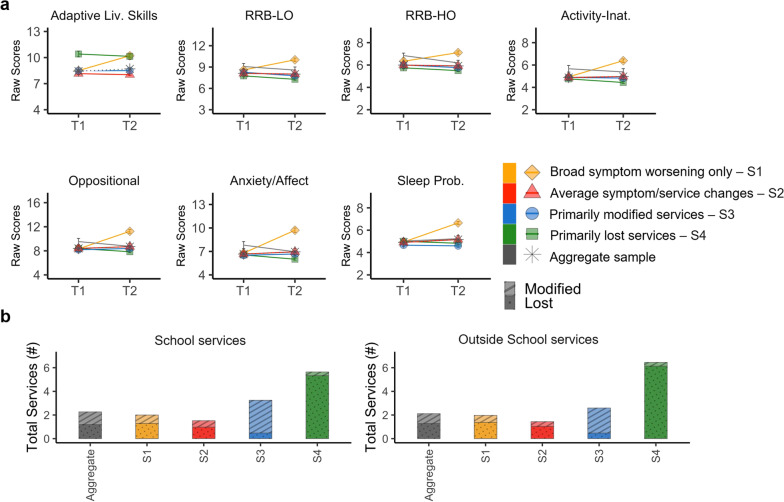
Results: Clustering revealed four subgroups. One subgroup-broad symptom worsening only (20%)-included youth with worsening across a range of symptoms but with service disruptions similar to the average of the aggregate sample. The other three subgroups were, relatively, clinically stable but differed in service access: primarily modified services (23%), primarily lost services (6%), and average services/symptom changes (53%). Distinct combinations of a set of pre-pandemic services, pandemic environment (e.g., COVID-19 new cases, restrictions), experiences (e.g., COVID-19 Worries), and age predicted each outcome subgroup.
Limitations: Notable limitations of the study are its cross-sectional nature and focus on the first six months of the pandemic.
Conclusions: Concomitantly assessing variation in changes of symptoms and service access during the first phase of the pandemic revealed differential outcome profiles in ASD/NDD youth. Subgroups were characterized by distinct prediction patterns across a set of pre- and pandemic-related experiences/contexts. Results may inform recovery efforts and preparedness in future crises; they also underscore the critical value of international data-sharing and collaborations to address the needs of those most vulnerable in times of crisis.
Keywords: Autism spectrum disorder; Behavioral problems; COVID-19 pandemic; Mental health outcomes; Neurodevelopmental conditions; Prediction; Public health; Risk and resilience factors; Sleep.
© 2023. The Author(s).
Conflict of interest statement
Dr. Bishop receives royalties for the sale of the ADOS-2 that she has co-authored. Royalties generated from any of their own research or clinical activities are donated to charity. Dr. Tancredi receives royalties for the sale of the Italian version of the ADOS-2. The other authors declare that they have no competing interests.
Figures
References
-
- Unite Nations. Policy Brief: The Impact of COVID-19 on Children. UN; 2020.
-
- Child Protection and COVID-19. Accessed November 3, 2022. https://alliancecpha.org/en/child-protection-and-covid-19.
-
- World Health Organization. The international statistical classification of diseases and health related problems ICD-10: tenth revision. Volume 2: Instruction Manual. World Health Organization; 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
