

Phenobarbital and Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis
- PMID: 36788902
- PMCID: PMC9922035
- DOI: 10.7759/cureus.33695
Phenobarbital and Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis
Abstract
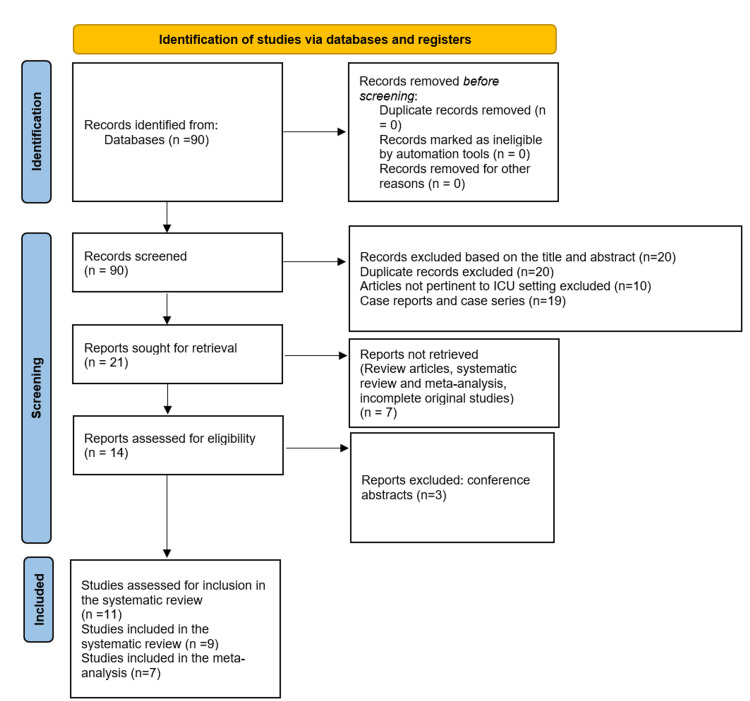
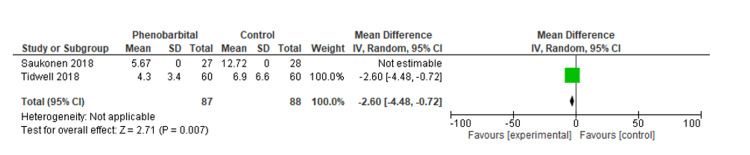
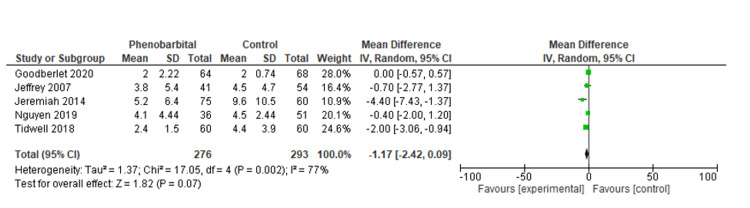
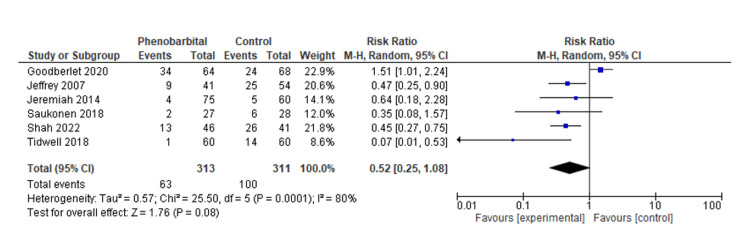
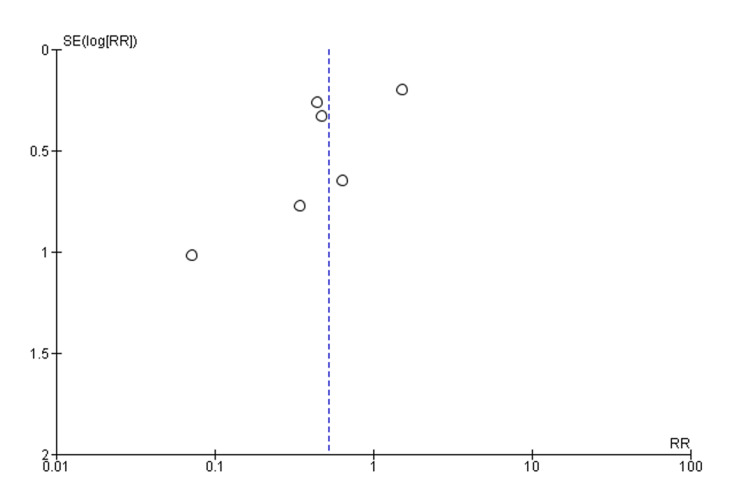
Alcohol withdrawal syndrome (AWS) is a complication frequently encountered among patients who are chronic alcohol abusers. It is considered to have a significant impact on the United States healthcare system. It not only has a toll on the healthcare spending but also contributes to significant morbidity and mortality. Benzodiazepines are considered first line in the treatment of AWS. Since patients with alcohol use disorder have downregulated gamma aminobutyric acid (GABA) receptors, this often leads to benzodiazepine resistance. Phenobarbital is also used in the management of alcohol withdrawal syndrome. Here we present a systematic review and meta-analysis of the efficacy and safety of the drug. We conducted an electronic database search for relevant studies published between the inception of the project and November 20, 2022, in three databases, including Medline/PubMed, Embase, and Cochrane Library. Our study included all original studies with prime focus on the baseline characteristics of patients admitted to the intensive care unit (ICU) for alcohol withdrawal syndrome and management/monitoring protocol implemented for its treatment. The primary outcomes that were the focus of our study consisted of changes in the length of hospital stay, length of ICU stay, and changes in scoring systems (for alcohol withdrawal assessment and monitoring) following the implementation of phenobarbital. The secondary outcomes included complications such as intubation and mortality. Based on our analysis, the mean difference in hospital stay was statistically significant at -2.6 (95% CI, -4.48, -0.72, P=0.007) for phenobarbital compared to the benzodiazepine group. We were unable to comment on the heterogeneity in our meta-analysis due to the standard deviation not being reported in one study. There was no statistically significant difference regarding the length of stay in the intensive care unit compared to the control/comparative arm, with a mean difference of -1.17 (95% CI, -1.17, 0.09, P=0.07), with considerable heterogeneity (I2=77%, P=0.002). Our meta-analysis also investigated the risk of intubation between the phenobarbital and the control/comparative group. There was statistically significant difference in the incidence of intubation, relative risk (RR) 0.52 (95% CI, 0.25, 1.08, P=0.08), with considerable heterogeneity (I2=80%, P=0.0001). Our study concludes that phenobarbital is an effective tool in the management of AWS in an ICU setting. However, various studies have reported contradictory results, and vital information appears to be lacking. Moreover, there is a lack of uniformity in terms of phenobarbital dosing. Drug administration should be adapted according to the severity of the symptoms. Further studies need to be conducted discussing the safety profile and adverse effects of the drug when it comes to the management of alcohol withdrawal syndrome.
Keywords: alcohol withdrawal syndrome; icu patients; intratracheal intubation; length of stay in icu; phenobarbital therapy.
Copyright © 2023, Umar et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Adjunctive phenobarbital for alcohol withdrawal syndrome: a focused literature review. Murphy JA, Curran BM, Gibbons WA 3rd, Harnica HM. Ann Pharmacother. 2021;55:1515–1524. - PubMed
-
- Management of drug and alcohol withdrawal. Kosten TR, O'Connor PG. N Engl J Med. 2003;348:1786–1795. - PubMed
-
- The ASAM Clinical Practice Guideline on alcohol withdrawal management. J Addict Med. 2020;14:1–72. - PubMed
Publication types
LinkOut - more resources
Full Text Sources