

Renal denervation in the management of hypertension in adults. A clinical consensus statement of the ESC Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI)
- PMID: 36789560
- PMCID: PMC10020821
- DOI: 10.4244/EIJ-D-22-00723
Renal denervation in the management of hypertension in adults. A clinical consensus statement of the ESC Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI)
Abstract
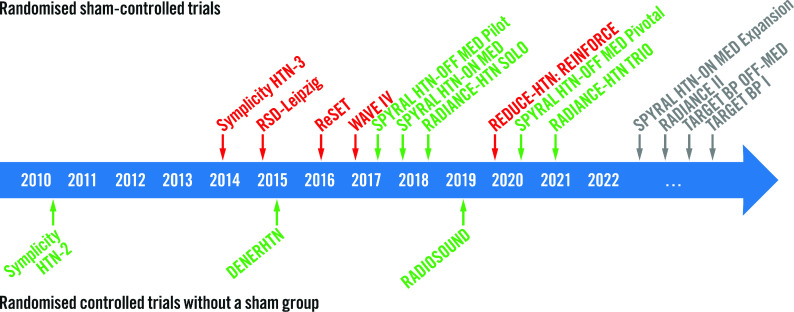
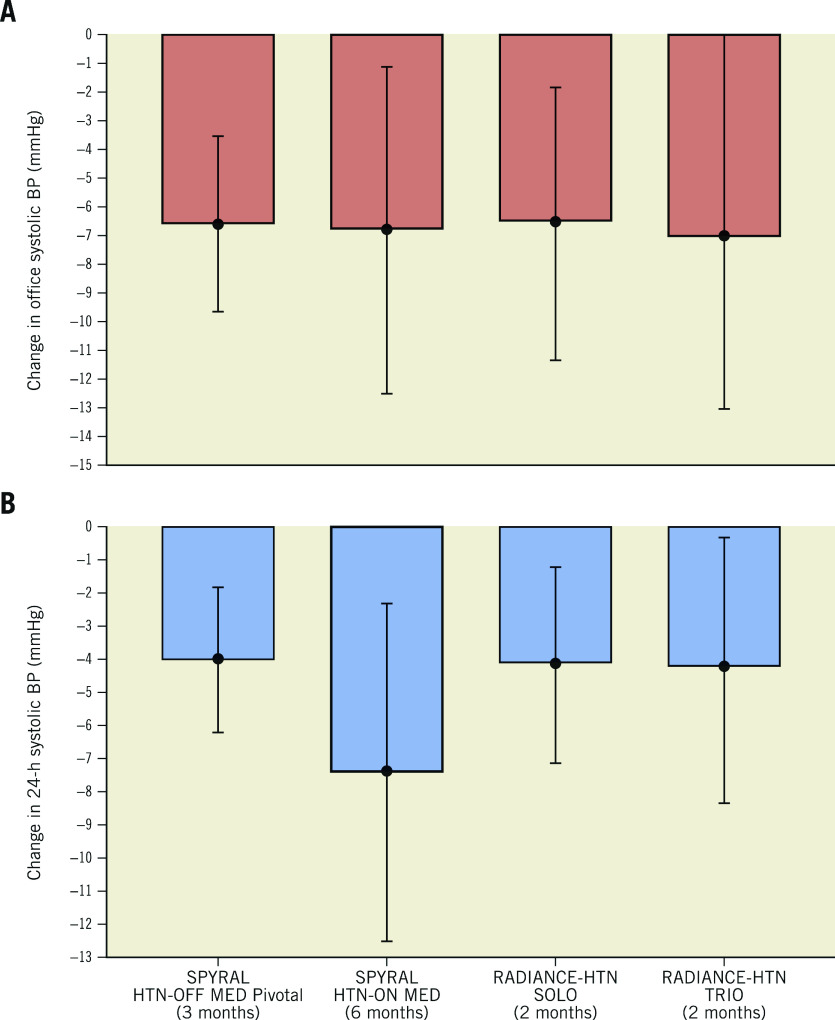
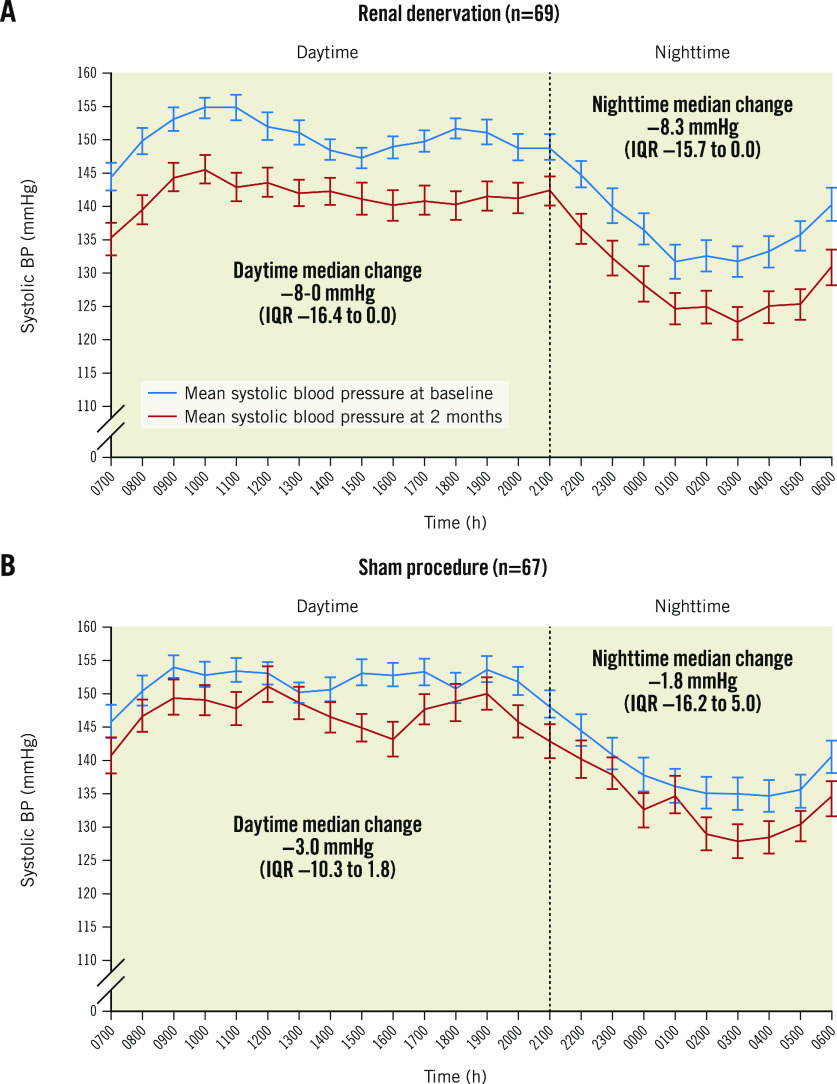
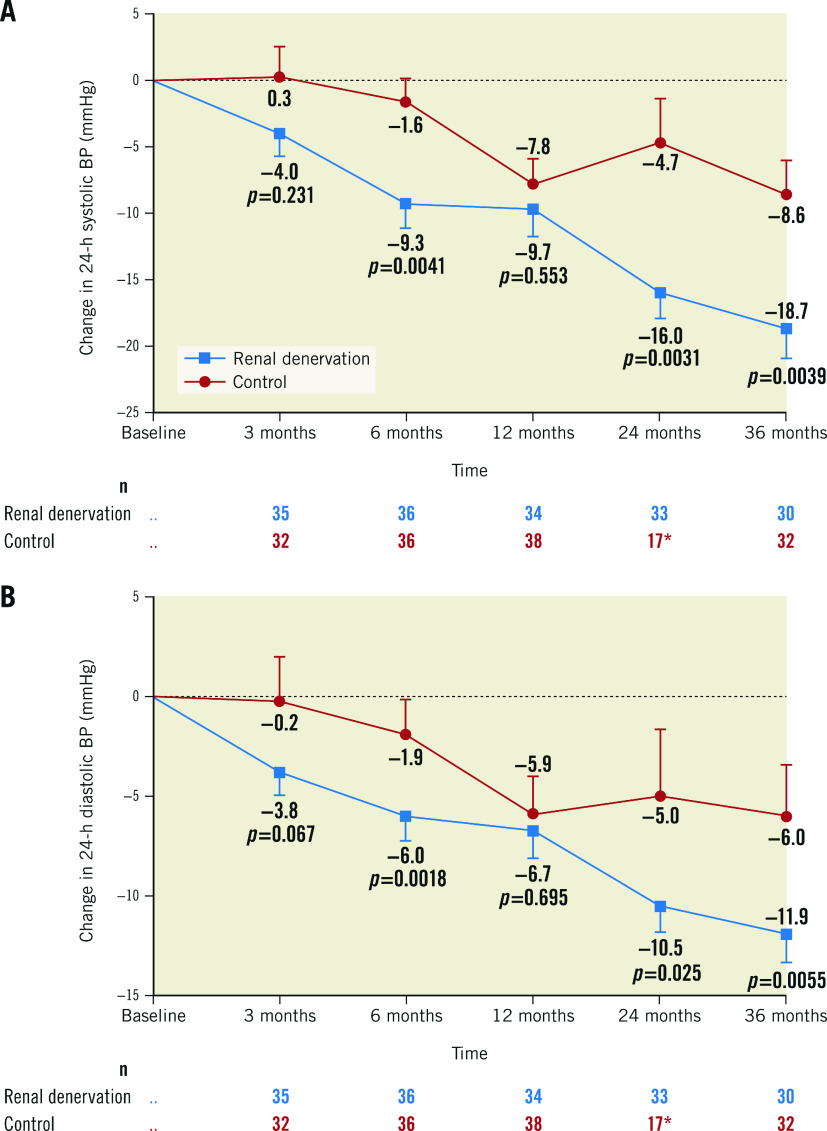
Since the publication of the 2018 European Society of Cardiology/European Society of Hypertension (ESC/ESH) Guidelines for the Management of Arterial Hypertension, several high-quality studies, including randomised, sham-controlled trials on catheter-based renal denervation (RDN) were published, confirming both the blood pressure (BP)-lowering efficacy and safety of radiofrequency and ultrasound RDN in a broad range of patients with hypertension, including resistant hypertension. A clinical consensus document by the ESC Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI) on RDN in the management of hypertension was considered necessary to inform clinical practice. This expert group proposes that RDN is an adjunct treatment option in uncontrolled resistant hypertension, confirmed by ambulatory BP measurements, despite best efforts at lifestyle and pharmacological interventions. RDN may also be used in patients who are unable to tolerate antihypertensive medications in the long term. A shared decision-making process is a key feature and preferably includes a patient who is well informed on the benefits and limitations of the procedure. The decision-making process should take (i) the patient's global cardiovascular (CV) risk and/or (ii) the presence of hypertension-mediated organ damage or CV complications into account. Multidisciplinary hypertension teams involving hypertension experts and interventionalists evaluate the indication and facilitate the RDN procedure. Interventionalists require expertise in renal interventions and specific training in RDN procedures. Centres performing these procedures require the skills and resources to deal with potential complications. Future research is needed to address open questions and investigate the impact of BP-lowering with RDN on clinical outcomes and potential clinical indications beyond hypertension.
Conflict of interest statement
E. Barbato has received speaker honoraria from BSCI, Abbott, OpSens, and Insight Lifetech. M. Azizi has received grant support and non-financial support from ReCor Medical and Idorsia; and has received consulting fees from Medtronic, AstraZeneca, Alnylam Pharmaceutical, Poxel Pharma, and Novartis. R.E. Schmieder has received scientific support and grants from Medtronic, ReCor Medical, and Ablative Solutions to the institution; has received honoraria for lectures from Ablative Solutions, Apontis, AstraZeneca, Bayer, Boehringer Ingelheim, Lilly, MENARINI, Medtronic, Novo Nordisk, Novartis, ReCor Medical, and Servier; and honoraria for advisory board activities from Ablative Solutions, Apontis, AstraZeneca, Bayer, Boehringer Ingelheim, Lilly, MENARINI, Medtronic, Novo Nordisk, Novartis, ReCor Medical, and Servier. L. Lauder reports speaker honoraria from Medtronic and ReCor Medical. M. Böhm reports personal fees from Abbott, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Vifor, Servier, Medtronic, and Novartis; and grants from Deutsche Forschungsgemeinschaft and AstraZeneca. S. Brouwers has received speaker honoraria from Sanofi, Daiichi Sankyo, Servier, MENARINI, and Merck through the institution. R.M. Bruno is supported by H2020 InSiDe (grant agreement No 871547) and has received speaker honoraria from Medtronic. T. Kahan reports research grants to the Karolinska Institute from Medtronic and ReCor Medical, all outside the submitted work. D.E. Kandzari has received institutional research and grant support from Medtronic and Ablative solutions; personal consulting honoraria from Medtronic and Ablative Solutions; and has equity in BioStar Ventures, but none related to Ablative Solutions. T.F. Lüscher has recieved research and educational grants to the institution from Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Sanofi, Servier and Vifor, outside this work; and honoraria from Abbott India, Acthera, Cor2ED, Dacadoo, Daiichi Sankyo, Novo Nordisk and Pfizer, unrelated to this work. G. Parati reports speaker honoraria from Omron Healthcare, Bayer, and Servier. A. Pathak reports consultancy/speaker honoraria from Medtronic, ReCor Medical, and Ablative Solutions. F.L. Ribichini has received scientific support and speaker honoraria from Medtronic. M.P. Schlaich is supported by an NHMRC Research Fellowship and has received consulting fees, and/or travel and research support from Medtronic, Abbott, ReCor Medical, Novartis, Servier, Pfizer, and Boehringer Ingelheim. A.S.P. Sharp reports consultancy/speaker honoraria from Medtronic, ReCor Medical, Philips, and Boston Scientific. I. Sudano has received consulting fees from Amgen, AstraZeneca, Daiichi Sankyo, MSD, Medtronic, Novartis, Novo Nordisk, Recordati, Sanofi, and Servier; travel grants from Amgen, AstraZeneca, Daiichi Sankyo, MSD, Medtronic, Novartis, Novo Nordisk, Recordati, Sanofi, and Servier; and honoraria from Amgen, AstraZeneca, Daiichi Sankyo, MSD, Medtronic, Novartis, Novo Nordisk, Recordati, Sanofi, and Servier. M. Volpe has received honoraria from the speakers bureaus at AstraZeneca, Novartis, Boehringer Ingelheim, Bayer, and Amgen; has received payments for scientific collaborations from MENARINI, Servier, Novo Nordisk, Novartis, and Sanofi; has a contract of collaboration with Medtronic but did not receive fees; is a member of the Kalos Medical advisory board. C. Tsioufis has received grants or honoraria from Medtronic, ReCor Medical, AstraZeneca, Bayer, Boehringer Ingelheim, MENARINI, Elpen, Win Medica, Vianex, Novartis, and Servier. W. Wijns reports institutional grants and honoraria from MicroPort; and is the co-founder of Argonauts, an innovation facilitator. F. Mahfoud is supported by Deutsche Gesellschaft für Kardiologie (DGK), Deutsche Forschungsgemeinschaft (SFB TRR219), and Deutsche Herzstiftung. He has received scientific support (to the institution) from Ablative Solutions, Medtronic, and ReCor Medical; and speaker honoraria from Ablative Solutions, AstraZeneca, Bayer, Boehringer Ingelheim, Inari, Medtronic, Merck, and ReCor Medical. The other authors have no conflicts of interest to declare.
Figures
References
-
- Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, Chalmers J, Rodgers A, Rahimi K. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–67. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical