

Poorer sleep health is associated with altered brain activation during cognitive control processing in healthy adults
- PMID: 36790738
- PMCID: PMC10233256
- DOI: 10.1093/cercor/bhad024
Poorer sleep health is associated with altered brain activation during cognitive control processing in healthy adults
Abstract
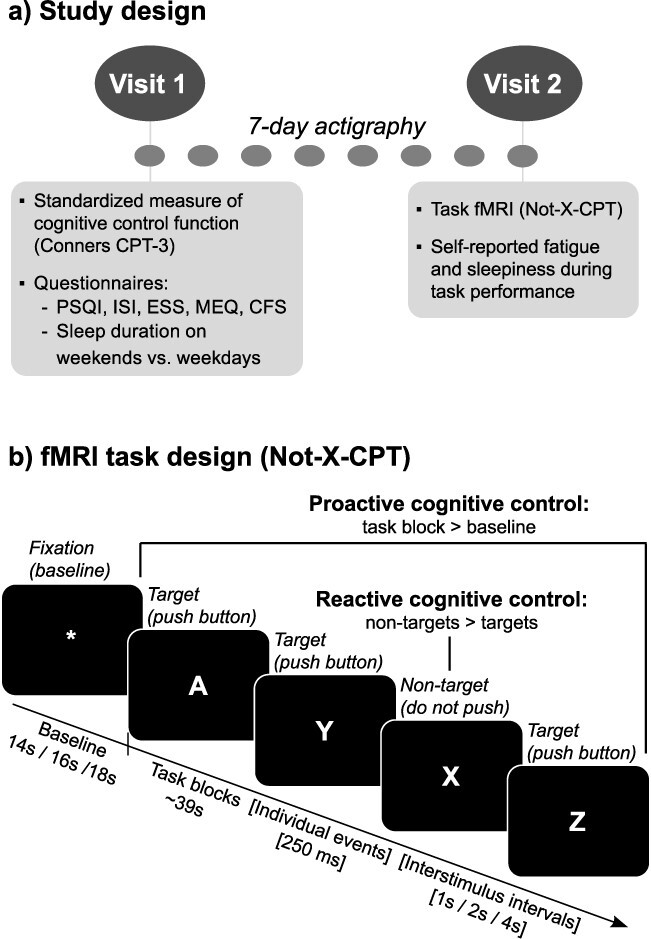
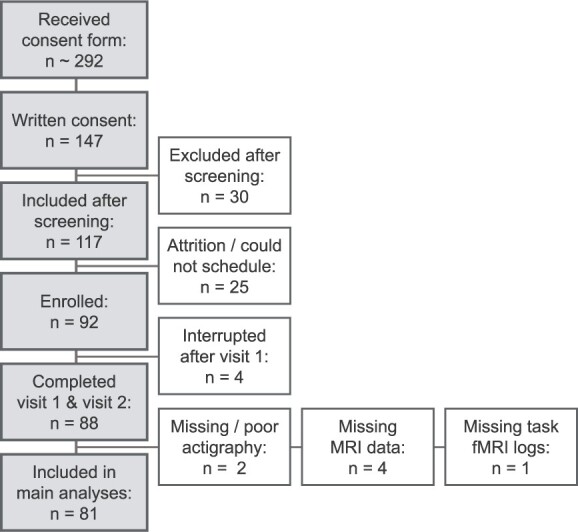
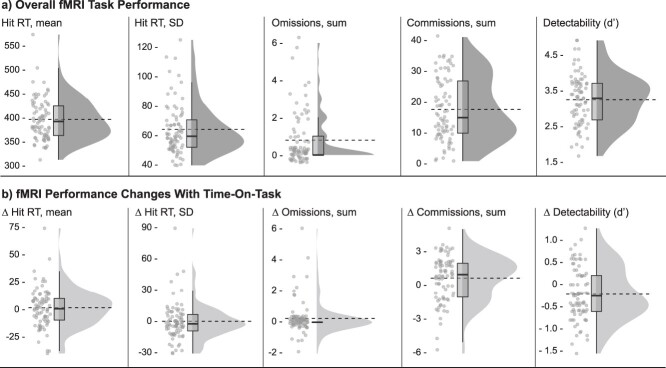
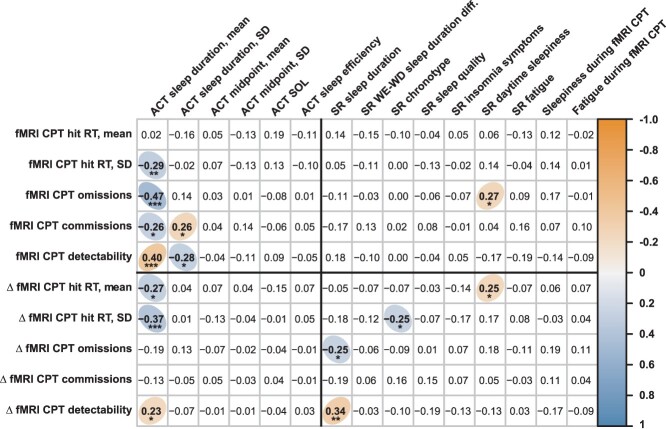
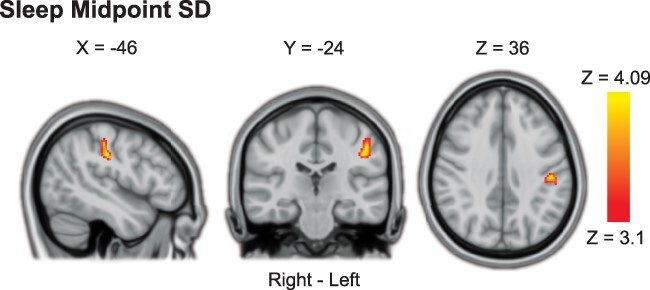
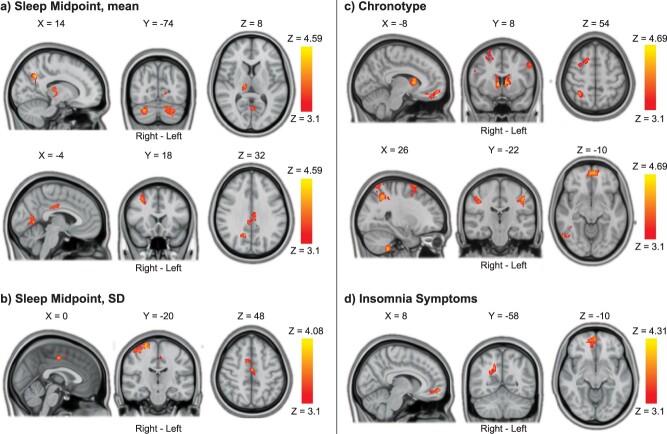
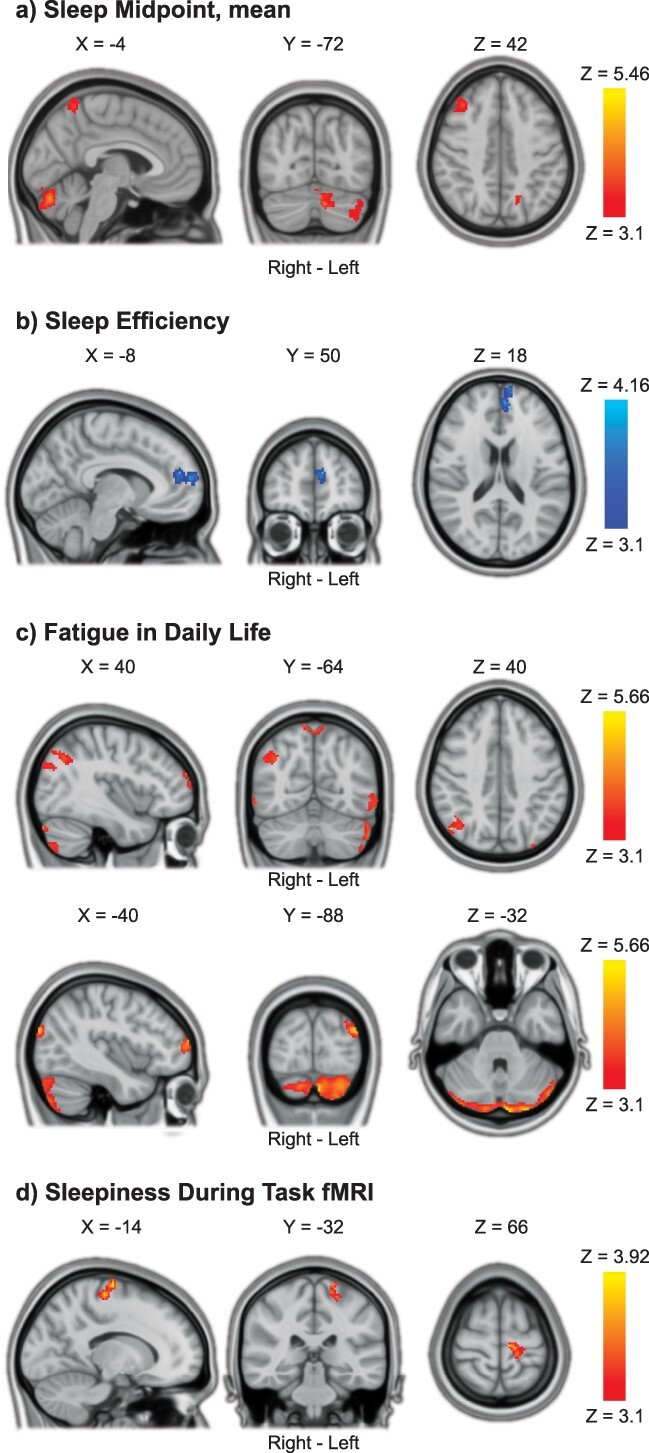
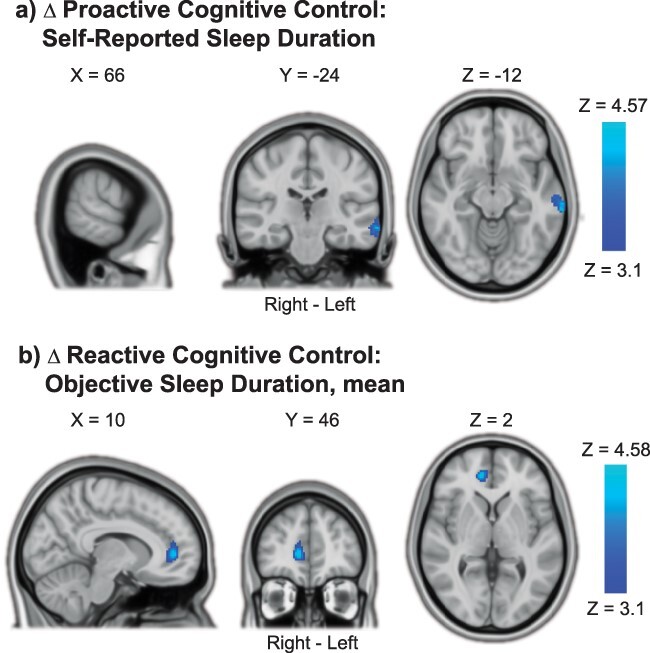
This study investigated how proactive and reactive cognitive control processing in the brain was associated with habitual sleep health. BOLD fMRI data were acquired from 81 healthy adults with normal sleep (41 females, age 20.96-39.58 years) during a test of cognitive control (Not-X-CPT). Sleep health was assessed in the week before MRI scanning, using both objective (actigraphy) and self-report measures. Multiple measures indicating poorer sleep health-including later/more variable sleep timing, later chronotype preference, more insomnia symptoms, and lower sleep efficiency-were associated with stronger and more widespread BOLD activations in fronto-parietal and subcortical brain regions during cognitive control processing (adjusted for age, sex, education, and fMRI task performance). Most associations were found for reactive cognitive control activation, indicating that poorer sleep health is linked to a "hyper-reactive" brain state. Analysis of time-on-task effects showed that, with longer time on task, poorer sleep health was predominantly associated with increased proactive cognitive control activation, indicating recruitment of additional neural resources over time. Finally, shorter objective sleep duration was associated with lower BOLD activation with time on task and poorer task performance. In conclusion, even in "normal sleepers," relatively poorer sleep health is associated with altered cognitive control processing, possibly reflecting compensatory mechanisms and/or inefficient neural processing.
Keywords: continuous performance test; executive function; magnetic resonance imaging; neuropsychology; sleep.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
PMT received partial grant support from Biogen, Inc., for research unrelated to this manuscript. AO is an owner and medical advisor for Nordic Brain Tech AS.
Figures
Similar articles
-
Brain activations elicited during task-switching generalize beyond the task: A partial least squares correlation approach to combine fMRI signals and cognition.Hum Brain Mapp. 2024 Aug 1;45(11):e26804. doi: 10.1002/hbm.26804. Hum Brain Mapp. 2024. PMID: 39126346 Free PMC article.
-
Age-related differences in BOLD modulation to cognitive control costs in a multitasking paradigm: Global switch, local switch, and compatibility-switch costs.Neuroimage. 2018 May 15;172:146-161. doi: 10.1016/j.neuroimage.2018.01.030. Epub 2018 Feb 3. Neuroimage. 2018. PMID: 29414492
-
Neural reward processing in self-reported short sleepers: examination of gambling task brain activation in the Human Connectome Project database.Sleep. 2019 Sep 6;42(9):zsz129. doi: 10.1093/sleep/zsz129. Sleep. 2019. PMID: 31152181 Free PMC article.
-
Preterm birth leads to hyper-reactive cognitive control processing and poor white matter organization in adulthood.Neuroimage. 2018 Feb 15;167:419-428. doi: 10.1016/j.neuroimage.2017.11.055. Epub 2017 Nov 27. Neuroimage. 2018. PMID: 29191480 Free PMC article.
-
Naturally occurring circadian rhythm and sleep duration are related to executive functions in early adulthood.J Sleep Res. 2018 Feb;27(1):113-119. doi: 10.1111/jsr.12581. Epub 2017 Jul 20. J Sleep Res. 2018. PMID: 28726307
Cited by
-
Better characterizing sleep beliefs for personalized sleep health promotion: the French sleep beliefs scale validation study.Front Public Health. 2024 Jan 11;11:1293045. doi: 10.3389/fpubh.2023.1293045. eCollection 2023. Front Public Health. 2024. PMID: 38274535 Free PMC article.
-
From Reward to Anhedonia-Dopamine Function in the Global Mental Health Context.Biomedicines. 2023 Sep 6;11(9):2469. doi: 10.3390/biomedicines11092469. Biomedicines. 2023. PMID: 37760910 Free PMC article. Review.
-
Sleep-wake behavior, perceived fatigability, and cognitive reserve in older adults.Alzheimers Dement. 2024 Jun;20(6):4020-4031. doi: 10.1002/alz.13802. Epub 2024 May 1. Alzheimers Dement. 2024. PMID: 38690777 Free PMC article.
-
Examining sleep health and its associations with technology use among older adults in Sweden: insights from a population-based study.BMC Public Health. 2025 Aug 22;25(1):2896. doi: 10.1186/s12889-025-23894-8. BMC Public Health. 2025. PMID: 40847298
References
-
- Akerstedt T, Gillberg M. Subjective and objective sleepiness in the active individual. Int J Neurosci. 1990:52:29–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
