

Seroprevalence of Antibodies to SARS-CoV-2 in Rural Households in Eastern Uganda, 2020-2022
- PMID: 36790811
- PMCID: PMC9932849
- DOI: 10.1001/jamanetworkopen.2022.55978
Seroprevalence of Antibodies to SARS-CoV-2 in Rural Households in Eastern Uganda, 2020-2022
Abstract
Importance: Estimating the true burden of SARS-CoV-2 infection has been difficult in sub-Saharan Africa owing to asymptomatic infections and inadequate testing capacity. Antibody responses from serologic surveys can provide an estimate of SARS-CoV-2 exposure at the population level.
Objective: To estimate SARS-CoV-2 seroprevalence, attack rates, and reinfection in eastern Uganda using serologic surveillance from 2020 to early 2022.
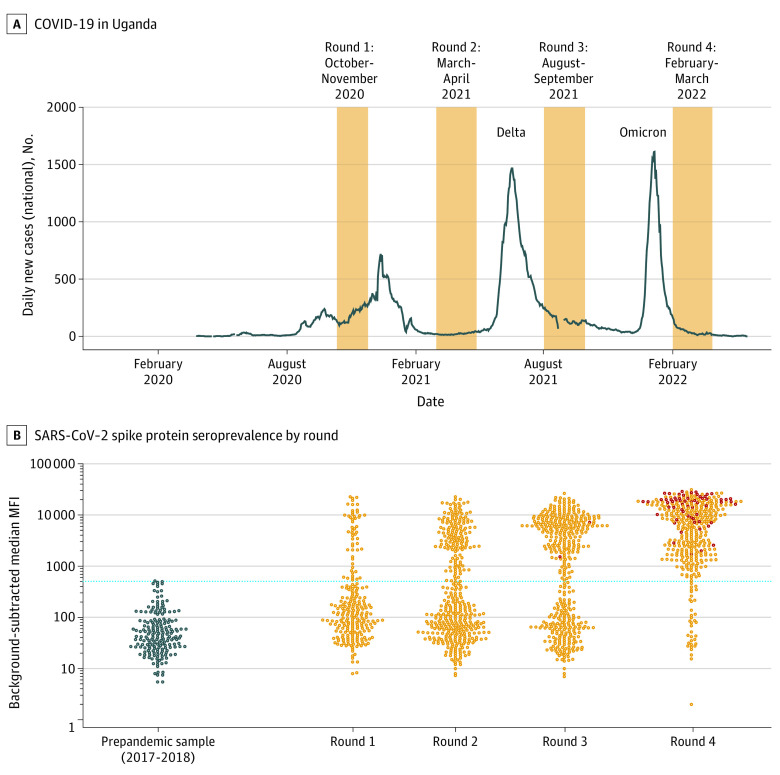
Design, setting, and participants: This cohort study was conducted in the Tororo and Busia districts of eastern Uganda. Plasma samples from participants in the Program for Resistance, Immunology, Surveillance, and Modeling of Malaria in Uganda Border Cohort were obtained at 4 sampling intervals: October to November 2020, March to April 2021, August to September 2021, and February to March 2022. Each participant contributed up to 4 time points for SARS-CoV-2 serology, with almost half of all participants contributing at all 4 time points, and almost 90% contributing at 3 or 4 time points. Information on SARS-CoV-2 vaccination status was collected from participants, with the earliest reported vaccinations in the cohort occurring in May 2021.
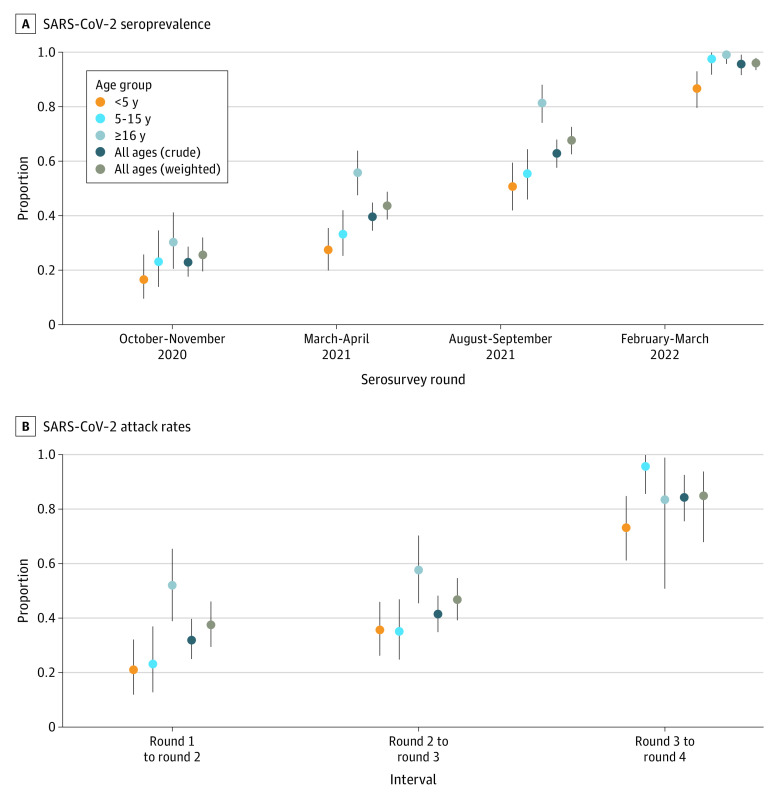
Main outcomes and measures: The main outcomes of this study were antibody responses to the SARS-CoV-2 spike protein as measured with a bead-based serologic assay. Individual-level outcomes were aggregated to population-level SARS-CoV-2 seroprevalence, attack rates, and boosting rates. Estimates were weighted by the local age distribution according to census data.
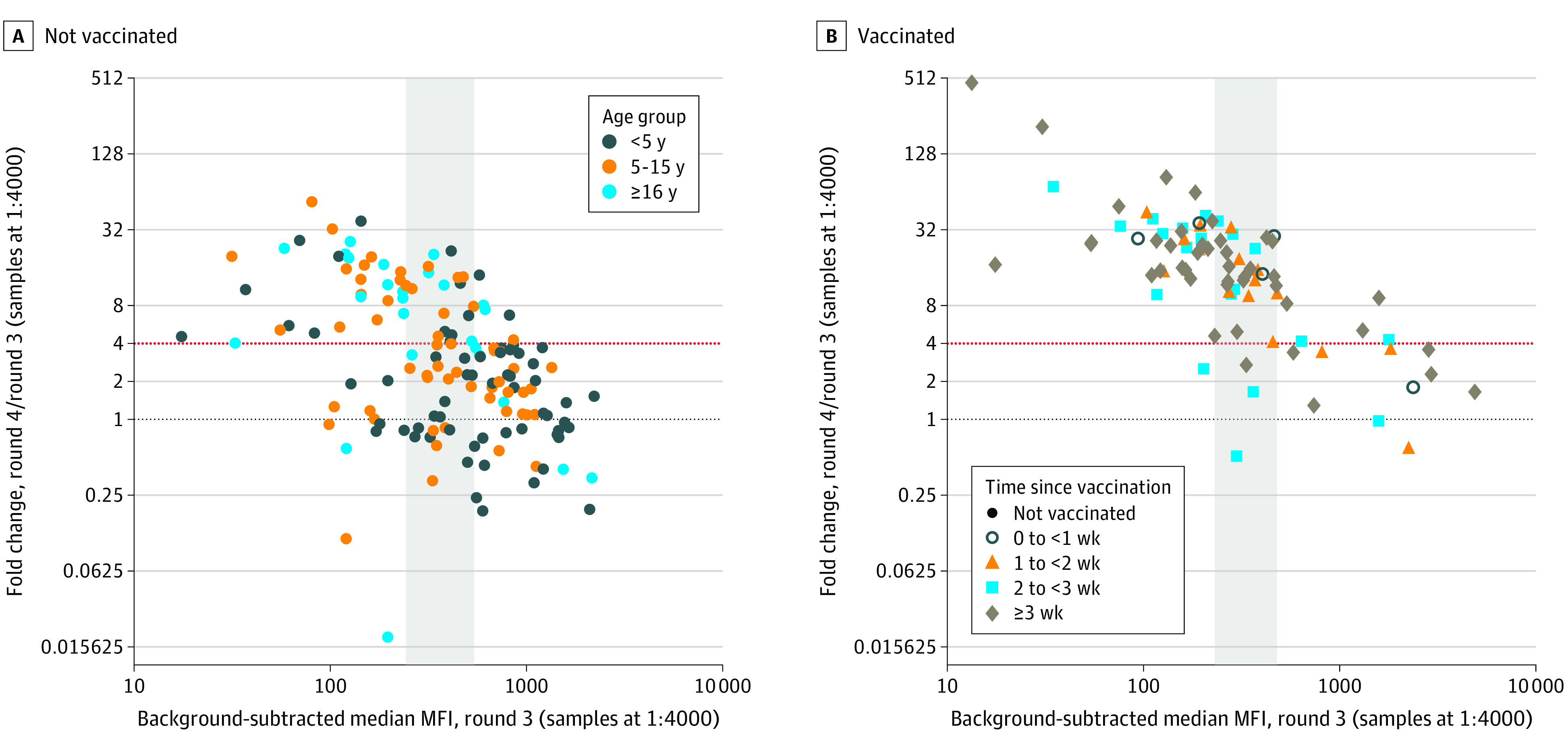
Results: A total of 1483 samples from 441 participants living in 76 households were tested. Of the 441 participants, 245 (55.6%) were female, and their mean (SD) age was 16.04 (16.04) years. By the end of the Delta wave and before widespread vaccination, adjusted SARS-CoV-2 seroprevalence was 67.7% (95% credible interval [CrI], 62.5%-72.6%) in the study population. During the subsequent Omicron wave, 84.8% (95% CrI, 67.9%-93.7%) of unvaccinated, previously seronegative individuals were infected for the first time, and 50.8% (95% CrI, 40.6%-59.7%) of unvaccinated, already seropositive individuals were likely reinfected, leading to an overall seropositivity of 96.0% (95% CrI, 93.4%-97.9%) in this population. These results suggest a lower probability of reinfection in individuals with higher preexisting antibody levels. There was evidence of household clustering of SARS-CoV-2 seroconversion. No significant associations were found between SARS-CoV-2 seroconversion and gender, household size, or recent Plasmodium falciparum malaria exposure.
Conclusions and relevance: In this cohort study in a rural population in eastern Uganda, there was evidence of very high SARS-CoV-2 infection rates throughout the pandemic inconsistent with national level case data and high reinfection rates during the Omicron wave.
Conflict of interest statement
Figures
References
-
- Emily AB, Barekye B, Bower H, et al. Population-based serosurveys for SARS-CoV-2: key findings from five African countries: November 2020 to June 2021. SSRN. Preprint posted online February 22, 2022. doi: 10.2139/ssrn.4040702 - DOI
-
- Nankabirwa J, Bousema T, Blanken SL, et al. Measures of malaria transmission, infection, and disease in an area bordering two districts with and without sustained indoor residual spraying of insecticide in Uganda. PLoS One. Published online December 30, 2022. doi: 10.1371/journal.pone.0279464 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
