

Hospital Outcomes of Community-Acquired SARS-CoV-2 Omicron Variant Infection Compared With Influenza Infection in Switzerland
- PMID: 36790812
- PMCID: PMC9932839
- DOI: 10.1001/jamanetworkopen.2022.55599
Hospital Outcomes of Community-Acquired SARS-CoV-2 Omicron Variant Infection Compared With Influenza Infection in Switzerland
Abstract
Importance: With the ongoing COVID-19 pandemic, it is crucial to assess the current burden of disease of community-acquired SARS-CoV-2 Omicron variant in hospitalized patients to tailor appropriate public health policies. Comparisons with better-known seasonal influenza infections may facilitate such decisions.
Objective: To compare the in-hospital outcomes of patients hospitalized with the SARS-CoV-2 Omicron variant with patients with influenza.
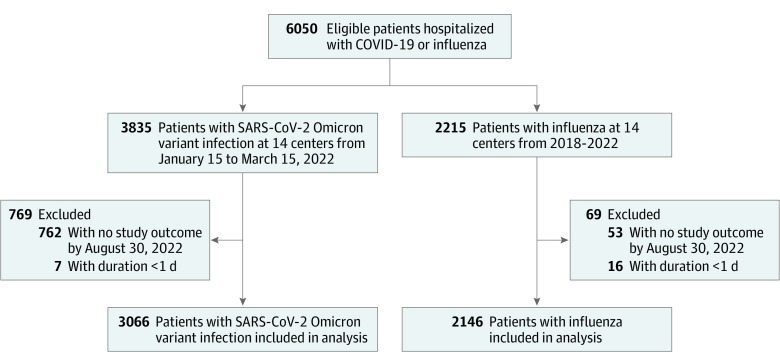
Design, setting, and participants: This cohort study was based on a national COVID-19 and influenza registry. Hospitalized patients aged 18 years and older with community-acquired SARS-CoV-2 Omicron variant infection who were admitted between January 15 and March 15, 2022 (when B.1.1.529 Omicron predominance was >95%), and hospitalized patients with influenza A or B infection from January 1, 2018, to March 15, 2022, where included. Patients without a study outcome by August 30, 2022, were censored. The study was conducted at 15 hospitals in Switzerland.
Exposures: Community-acquired SARS-CoV-2 Omicron variant vs community-acquired seasonal influenza A or B.
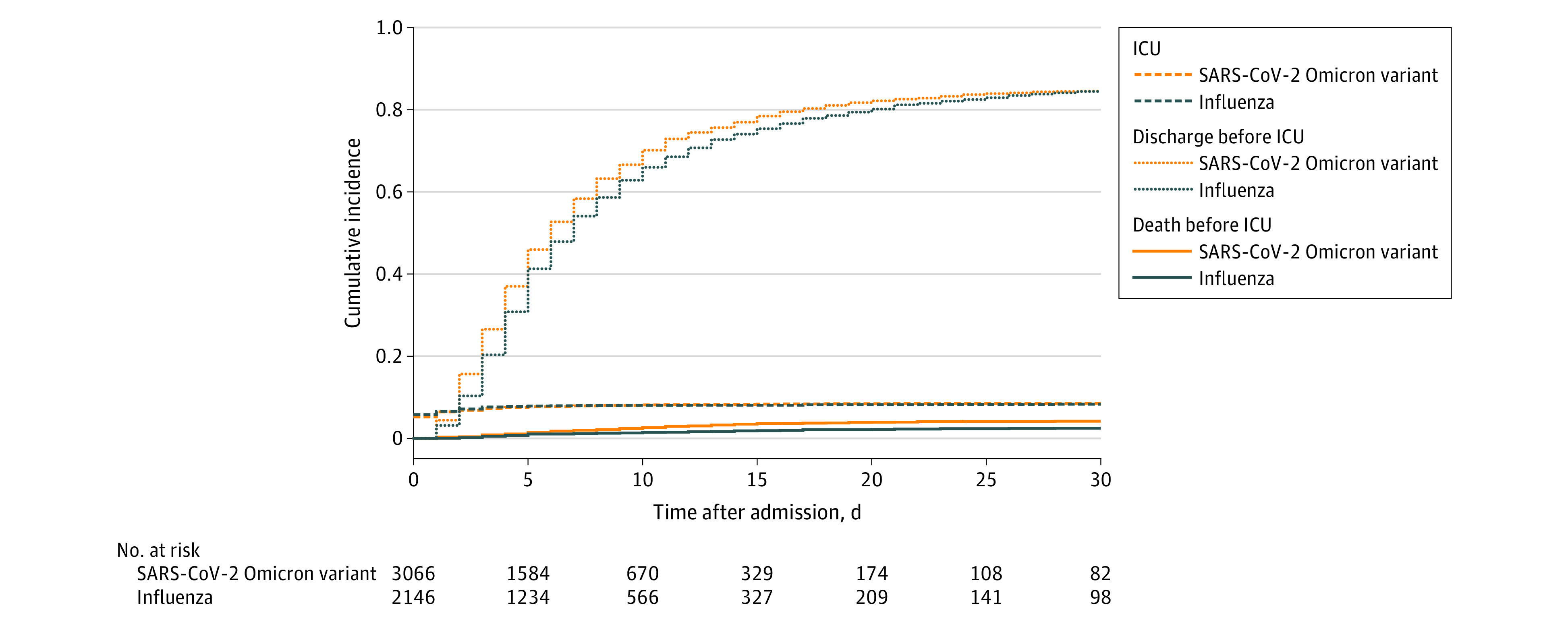
Main outcomes and measures: Primary and secondary outcomes were defined as in-hospital mortality and admission to the intensive care unit (ICU) for patients with the SARS-CoV-2 Omicron variant or influenza. Cox regression (cause-specific and Fine-Gray subdistribution hazard models) was used to account for time-dependency and competing events, with inverse probability weighting to adjust for confounders with right-censoring at day 30.
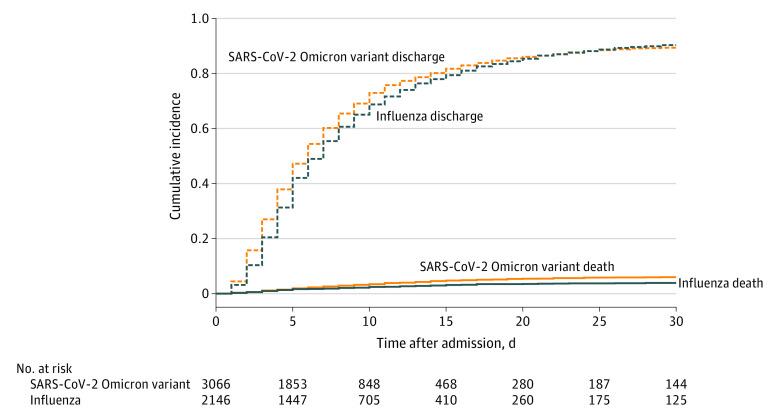
Results: Of 5212 patients included from 15 hospitals, 3066 (58.8%) had SARS-CoV-2 Omicron variant infection in 14 centers and 2146 patients (41.2%) had influenza A or B in 14 centers. Of patients with the SARS-CoV-2 Omicron variant, 1485 (48.4%) were female, while 1113 patients with influenza (51.9%) were female (P = .02). Patients with the SARS-CoV-2 Omicron variant were younger (median [IQR] age, 71 [53-82] years) than those with influenza (median [IQR] age, 74 [59-83] years; P < .001). Overall, 214 patients with the SARS-CoV-2 Omicron variant (7.0%) died during hospitalization vs 95 patients with influenza (4.4%; P < .001). The final adjusted subdistribution hazard ratio (sdHR) for in-hospital death for SARS-CoV-2 Omicron variant vs influenza was 1.54 (95% CI, 1.18-2.01; P = .002). Overall, 250 patients with the SARS-CoV-2 Omicron variant (8.6%) vs 169 patients with influenza (8.3%) were admitted to the ICU (P = .79). After adjustment, the SARS-CoV-2 Omicron variant was not significantly associated with increased ICU admission vs influenza (sdHR, 1.08; 95% CI, 0.88-1.32; P = .50).
Conclusions and relevance: The data from this prospective, multicenter cohort study suggest a significantly increased risk of in-hospital mortality for patients with the SARS-CoV-2 Omicron variant vs those with influenza, while ICU admission rates were similar.
Conflict of interest statement
Figures
References
-
- Nyberg T, Ferguson NM, Nash SG, et al. ; COVID-19 Genomics UK (COG-UK) consortium . Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 Omicron (B.1.1.529) and Delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022;399(10332):1303-1312. doi: 10.1016/S0140-6736(22)00462-7 - DOI - PMC - PubMed
-
- Bundesamt für Gesundheit . COVID-19 Schweiz. Updated March 20, 2022. Accessed March 20, 2022. https://www.covid19.admin.ch/de/epidemiologic/virus-variants
-
- World Health Organization . Classification of Omicron (B.1.1.529): SARS-CoV-2 variant of concern. Accessed July 20, 2022. https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1....
-
- Lewnard JA, Hong VX, Patel MM, Kahn R, Lipsitch M, Tartof SY. Clinical outcomes among patients infected with Omicron (B.1.1.529) SARS-CoV-2 variant and BA.1/BA.1.1 or BA.2 subvariant infection in southern California. Nat Med. 2022;28(9):1933-1943. doi: 10.1038/s41591-022-01887-z - DOI - PMC - PubMed
-
- Veneti L, Bøås H, Bråthen Kristoffersen A, et al. Reduced risk of hospitalisation among reported COVID-19 cases infected with the SARS-CoV-2 Omicron BA.1 variant compared with the Delta variant, Norway, December 2021 to January 2022. Euro Surveill. 2022;27(4):2200077. doi: 10.2807/1560-7917.ES.2022.27.4.2200077 - DOI - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
