

Guideline-Directed Medical Therapy and Long-Term Mortality and Amputation Outcomes in Patients Undergoing Peripheral Vascular Interventions
- PMID: 36792257
- PMCID: PMC10359106
- DOI: 10.1016/j.jcin.2022.09.022
Guideline-Directed Medical Therapy and Long-Term Mortality and Amputation Outcomes in Patients Undergoing Peripheral Vascular Interventions
Abstract
Background: Lack of guideline-directed medical therapy (GDMT) in patients undergoing peripheral vascular interventions (PVIs) may increase mortality and amputation risk.
Objectives: The authors sought to study the association between GDMT and mortality/amputation and to examine GDMT variability among providers and health systems.
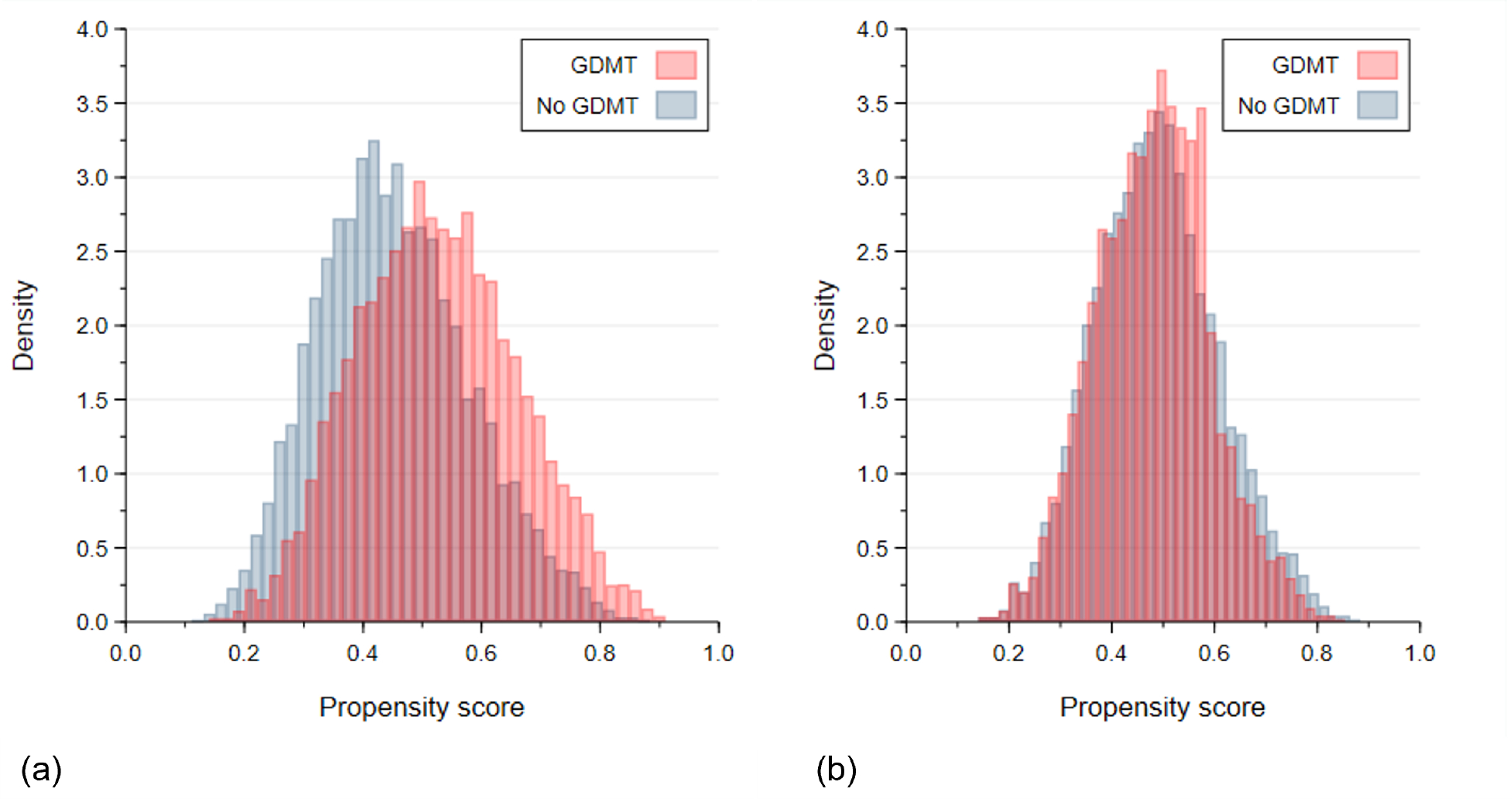
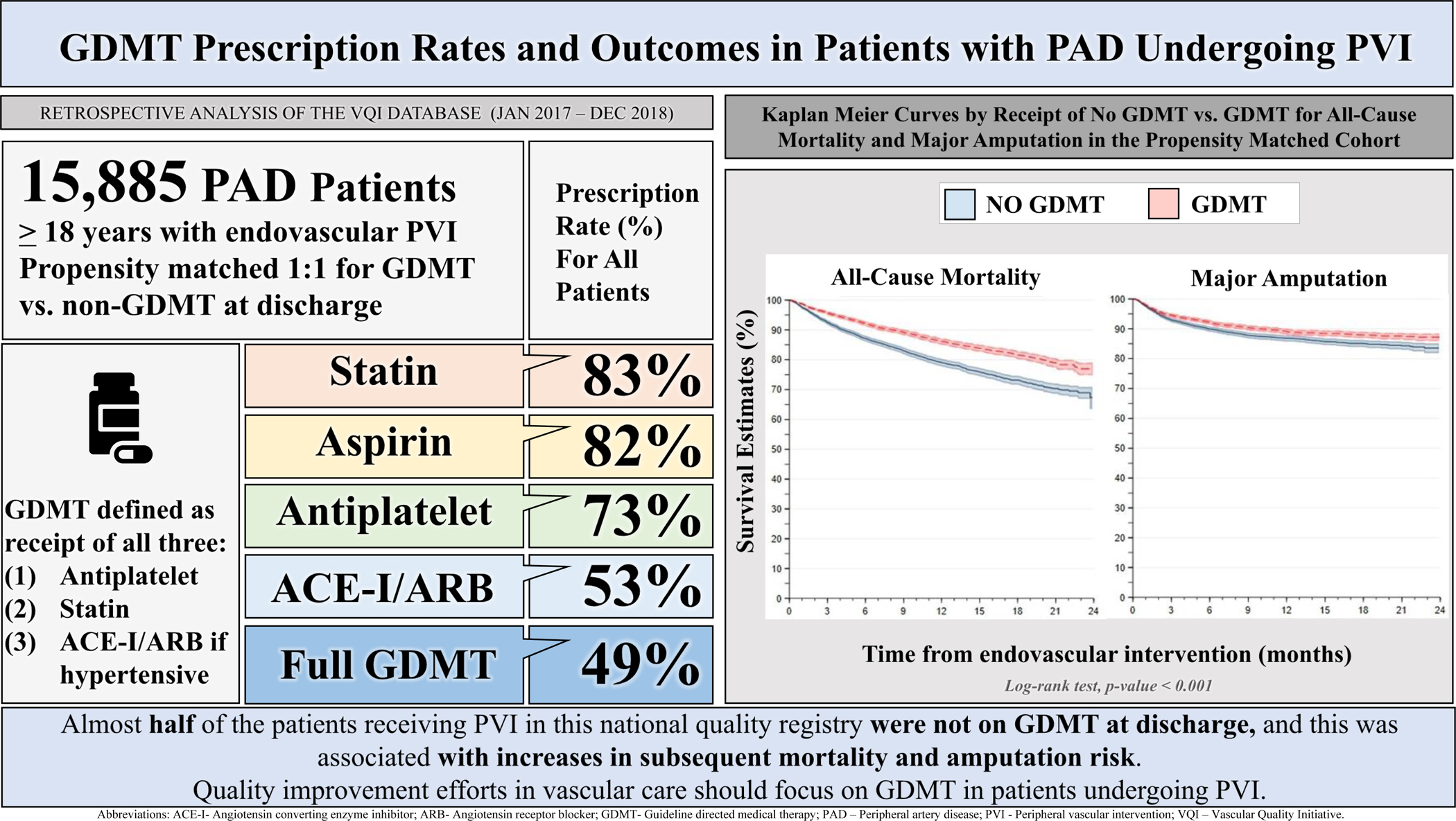
Methods: We performed an observational study using patients in the Vascular Quality Initiative registry undergoing PVI between 2017 and 2018. Two-year all-cause mortality and major amputation data were derived from Medicare claims data. Compliance with GDMT was defined as receiving a statin, antiplatelet therapy, and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker if hypertensive. Propensity 1:1 matching was applied for GDMT vs no GDMT and survival analyses were performed to compare outcomes between groups.
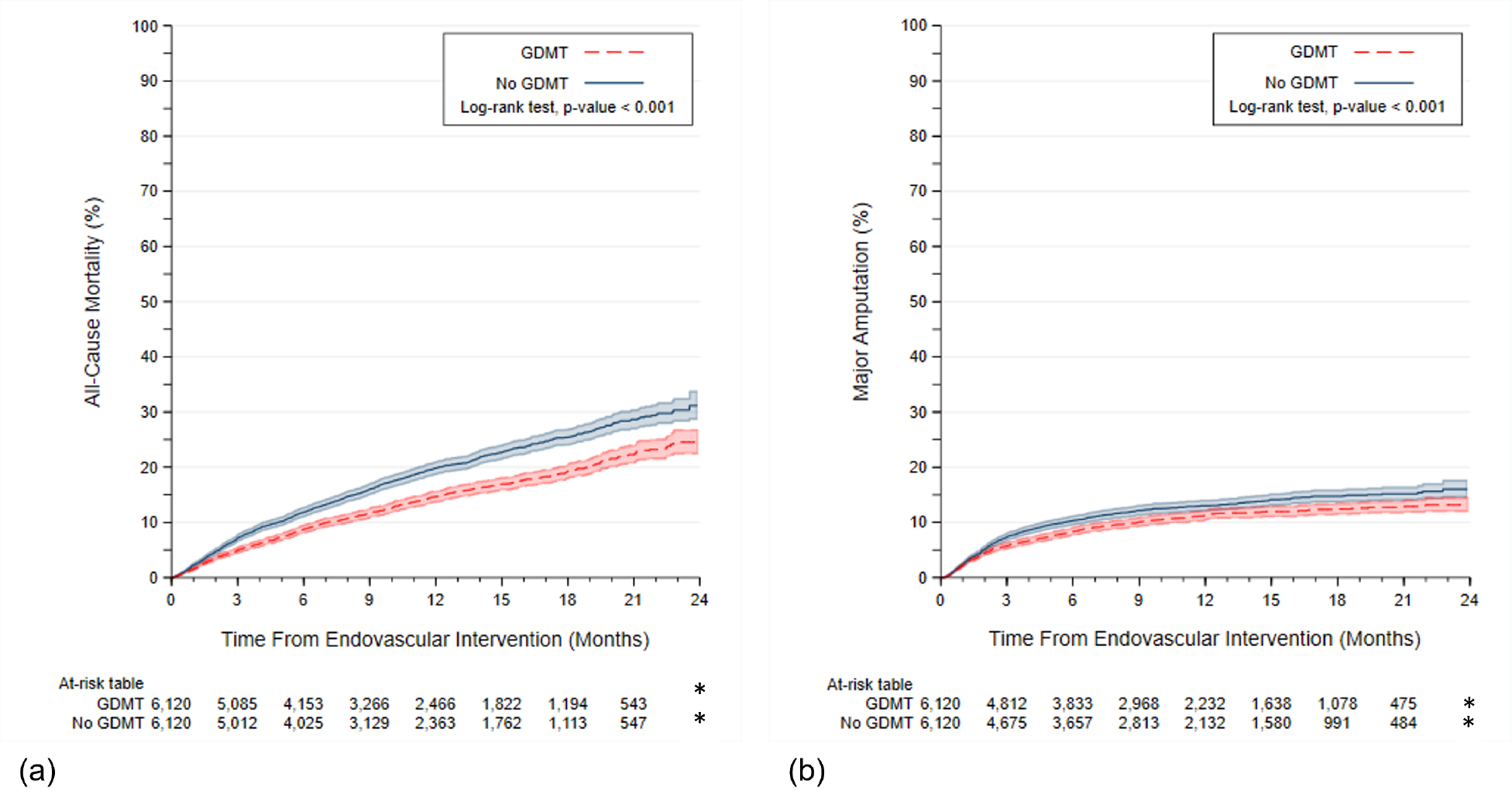
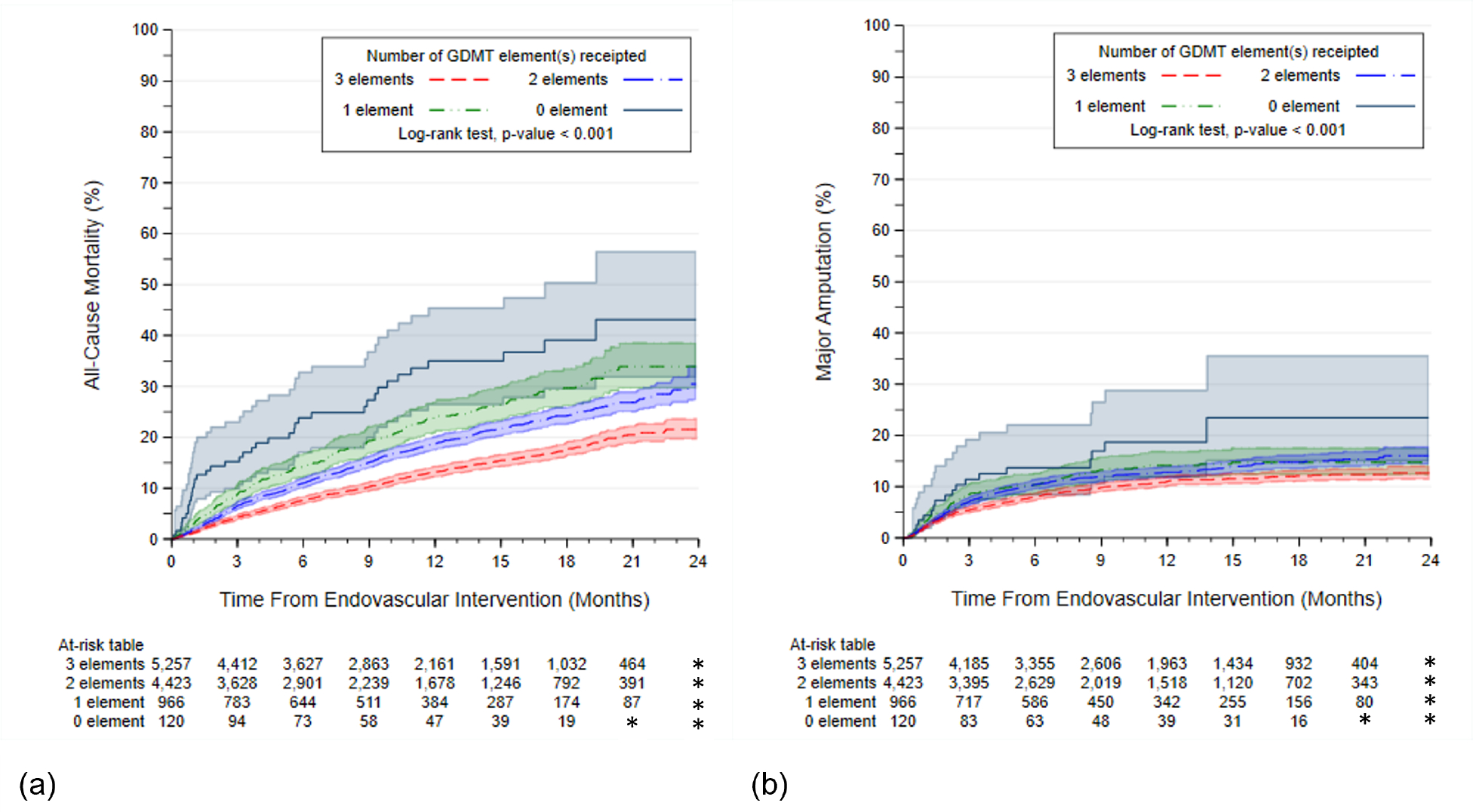
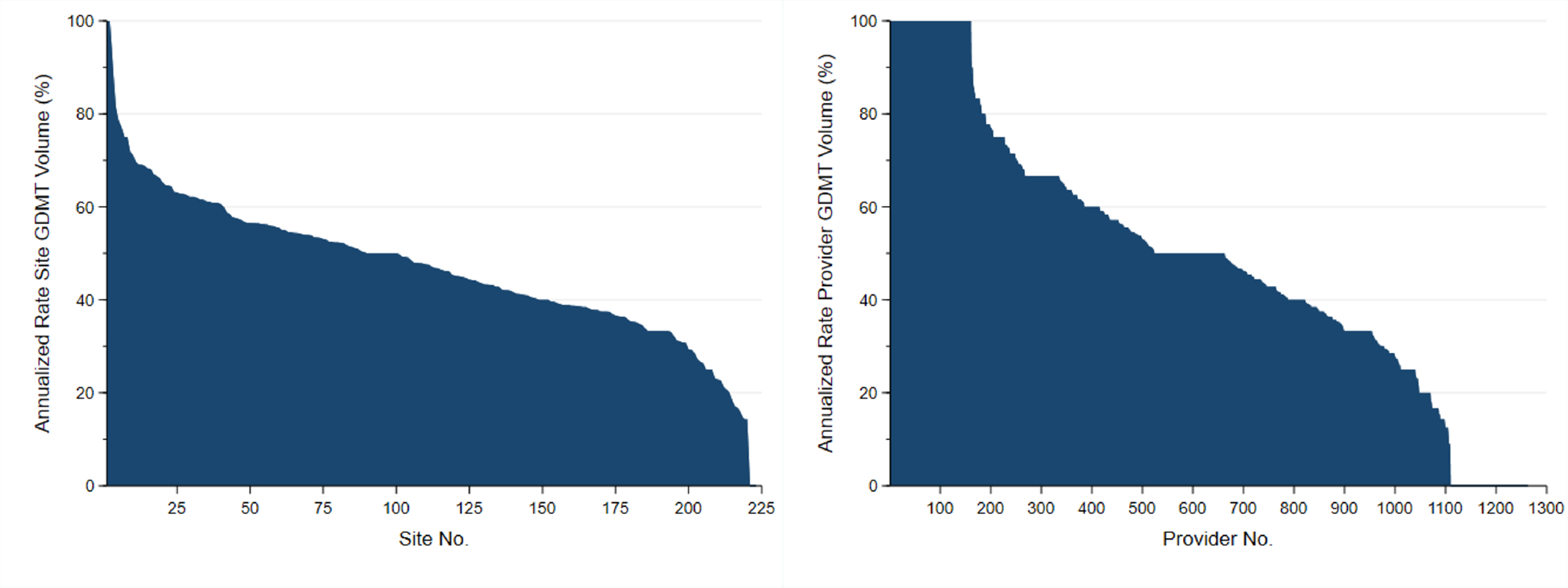
Results: Of 15,891 patients undergoing PVIs, 48.8% received GDMT and 6,120 patients in each group were matched. Median follow-up was 9.6 (IQR: 4.5-16.2) months for mortality and 8.4 (IQR: 3.5-15.4) for amputation. Mean age was 72.0 ± 9.9 years. Mortality risk was higher among patients who did not receive GDMT versus those on GDMT (31.2% vs 24.5%; HR: 1.37, 95% CI: 1.25-1.50; P < 0.001), as well as, risk of amputation (16.0% vs 13.2%; HR: 1.20; 95% CI: 1.08-1.35; P < 0.001). GDMT rates across sites and providers ranging from 0% to 100%, with lower performance translating into higher risk.
Conclusions: Almost one-half of the patients receiving PVI in this national quality registry were not on GDMT, and this was associated with increased risk of mortality and major amputation. Quality improvement efforts in vascular care should focus on GDMT in patients undergoing PVI.
Keywords: guideline-directed medical therapy; outcomes research; peripheral artery disease; quality of care.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The VISION registry was supported by a Food and Drug Administration grant (U01FD006936). Dr Mao is supported by a K01 award by the National Heart, Lung, and Blood Institute K01HL159315-01. Dr Goodney is supported by research grants from the American Heart Association (SRFN #18SFRN33900147 and a Food and Drug Administration grant (U01FD006936). Dr Smolderen has received unrestricted research grants from Merck & Co., Shockwave Medical, and Janssen Pharmaceutical Companies of Johnson & Johnson, Philips, Abbott, Merck; and served as a consultant for Optum Labs, Happify, Tegum, and Abbott Laboratories. Dr Mena-Hurtado has received grant funding from Shockwave Medical, Philips, Abbott, and served as a consultant for Abbott Laboratories, Cook Medical, Penumbra, and Optum Labs. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Guideline-Directed Medical Therapy in PAD: Time to Step on the Gas.JACC Cardiovasc Interv. 2023 Feb 13;16(3):344-346. doi: 10.1016/j.jcin.2022.10.015. JACC Cardiovasc Interv. 2023. PMID: 36792258 No abstract available.
Similar articles
-
Variability in guideline-directed medical therapy across sites and operators and long-term mortality and amputation outcomes risk in patients undergoing peripheral vascular interventions.Am Heart J. 2024 Apr;270:75-85. doi: 10.1016/j.ahj.2024.01.008. Epub 2024 Feb 1. Am Heart J. 2024. PMID: 38307364
-
Guideline-Directed Medical Therapy in Patients with Chronic Kidney Disease Undergoing Peripheral Vascular Intervention.Am J Nephrol. 2021;52(10-11):845-853. doi: 10.1159/000519484. Epub 2021 Oct 27. Am J Nephrol. 2021. PMID: 34706363
-
Predictors of Underutilization of Medical Therapy in Patients Undergoing Endovascular Revascularization for Peripheral Artery Disease.JACC Cardiovasc Interv. 2020 Dec 28;13(24):2911-2918. doi: 10.1016/j.jcin.2020.08.036. JACC Cardiovasc Interv. 2020. PMID: 33357529
-
The prevalence, predictors and outcomes of guideline-directed medical therapy in patients with acute myocardial infarction undergoing PCI, an analysis from the PROMETHEUS registry.Catheter Cardiovasc Interv. 2019 Feb 15;93(3):E112-E119. doi: 10.1002/ccd.27860. Epub 2018 Oct 23. Catheter Cardiovasc Interv. 2019. PMID: 30351514
-
Guideline-directed medical therapy for HFrEF: sequencing strategies and barriers for life-saving drug therapy.Heart Fail Rev. 2023 Sep;28(5):1221-1234. doi: 10.1007/s10741-023-10325-2. Epub 2023 Jun 14. Heart Fail Rev. 2023. PMID: 37311917 Free PMC article. Review.
Cited by
-
Markers of optimal medical therapy are associated with improved limb outcomes after elective revascularization for intermittent claudication.J Vasc Surg. 2025 Jan;81(1):200-209.e3. doi: 10.1016/j.jvs.2024.08.033. Epub 2024 Aug 27. J Vasc Surg. 2025. PMID: 39208918
-
Multi-modality imaging for assessment of the microcirculation in peripheral artery disease: Bench to clinical practice.Am Heart J Plus. 2024 May 8;42:100400. doi: 10.1016/j.ahjo.2024.100400. eCollection 2024 Jun. Am Heart J Plus. 2024. PMID: 38779485 Free PMC article.
-
Focus on Prevention: Peripheral Arterial Disease and the Central Role of the Cardiologist.J Clin Med. 2023 Jun 28;12(13):4338. doi: 10.3390/jcm12134338. J Clin Med. 2023. PMID: 37445373 Free PMC article. Review.
-
Prognostic Factors Associated with 2-year Mortality in Patients with Intermittent Claudication Treated with Endovascular Therapy for Femoropopliteal Lesions: Results from the Multicenter PROCYON Study.J Atheroscler Thromb. 2025 Jul 1;32(7):863-872. doi: 10.5551/jat.65379. Epub 2024 Dec 25. J Atheroscler Thromb. 2025. PMID: 39721706 Free PMC article.
References
-
- Virani SS, Alonso A, Aparicio HJ et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021;143:e254–e743. - PubMed
-
- Heart Outcomes Prevention Evaluation Study I, Yusuf S, Sleight P et al. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med 2000;342:145–53. - PubMed
-
- Buchner N, Banas B, Kramer BK. Telmisartan, ramipril, or both in patients at high risk of vascular events. N Engl J Med 2008;359:426. - PubMed
-
- Steg PG, Bhatt DL, Wilson PW et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA 2007;297:1197–206. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
