

Can systemic immune inflammation index at admission predict in-hospital mortality in chronic kidney disease patients with SARS-CoV-2 infection?
- PMID: 36792308
- PMCID: PMC9922800
- DOI: 10.1016/j.nefroe.2021.09.009
Can systemic immune inflammation index at admission predict in-hospital mortality in chronic kidney disease patients with SARS-CoV-2 infection?
Abstract
Background and aim: Patients with chronic kidney disease (CKD) are susceptible to SARS-CoV-2 infection and more prone to develop severe disease. It is important to know predictors of poor outcomes to optimize the strategies of care.
Methods: 93 patients with CKD and 93 age-sex matched patients without CKD were included in the study. Data on demographic, clinical features, hematological indices and outcomes were noted and compared between the groups. Neutrophile to lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune inflammation index (SII) (platelet counts×neutrophil counts/lymphocyte counts) and lymphocyte-to-CRP ratio (LCR) were calculated on admission and the association of these markers with disease mortality in CKD patients was identified.
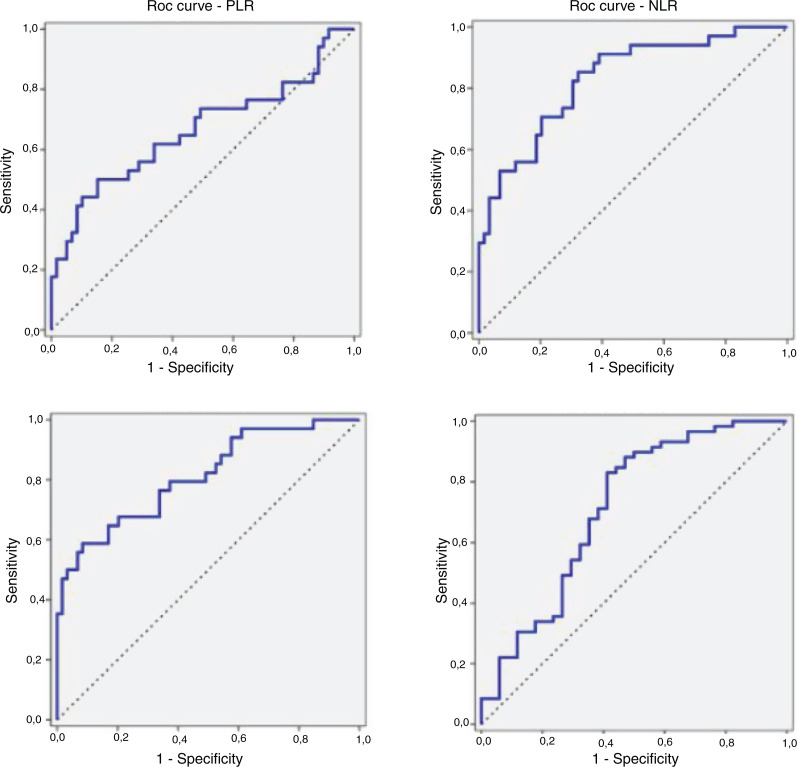
Results: CKD patients had higher risk of severe disease, and mortality compared to non-CKD patients (72% vs 50.5%, p=0.003, 36.6% vs 10.8%, p<0.001, respectively) and were more likely to have higher values of immuno-inflammatory indices (leukocyte count, neutrophil, NLR, SII and C-reactive protein, etc.) and lower level of lymphocyte and LCR. Also, higher levels of NLR, SII, PLR and lower level of LCR were seen in CKD patients who died compared to those recovered. In a receiver operating characteristic curve analysis, NLR, SII, PLR and LCR area under the curve for in-hospital mortality of CKD patients were 0.830, 0.811, 0.664 and 0.712, respectively. Among all parameters, NLR and SII gave us the best ability to distinguish patients with higher risk of death. Based on the cut-off value of 1180.5, the sensitivity and specificity of the SII for predicting in-hospital mortality were found to be 67.5% and 79.6%, respectively. The corresponding sensitivity and specificity of the NLR were 85.2% and 66.1%, respectively, at the cut-off value of 5.1. Forward stepwise logistic regression analysis showed that NLR (≥5.1), SII (≥1180.5) and LCR (≤9) were predictors for in-hospital mortality.
Conclusion: We report for the first time that SII is able to distinguish COVID-19 infected CKD patients of worse survival and it is as powerful as NLR in this regard. As SII is easily quantified from blood sample data, it may assist for early identification and timely management of CKD patients with worse survival.
Antecedentes y objetivo: Los pacientes con enfermedad renal crónica (ERC) son susceptibles a la infección por SARS-CoV-2 y más propensos a desarrollar una enfermedad grave. Es importante conocer los predictores de los malos resultados para optimizar las estrategias de atención.
Métodos: Se incluyeron en el estudio 93 pacientes con ERC y 93 pacientes sin ERC, emparejados por edad y sexo. Los datos sobre las características demográficas, clínicas, índices hematológicos y resultados, se anotaron y compararon entre los grupos. La proporción de neutrófilos a linfocitos (NLR), la proporción de plaquetas a linfocitos (PLR), el índice de inflamación inmunitaria sistémica (SII) (recuentos de plaquetas × recuentos de neutrófilos/recuentos de linfocitos) y la proporción de linfocitos a PCR (LCR) se calcularon en el momento de la admisión y se identificó la asociación de estos marcadores con la mortalidad por enfermedad en pacientes con ERC.
Resultados: Los pacientes con ERC tuvieron un mayor riesgo de enfermedad grave y mortalidad en comparación con los pacientes sin ERC (72% vs 50,5%, p = 0,003, 36,6% vs 10,8%, p < 0,001, respectivamente) y tuvieron más probabilidades de tener valores más altos de índices inmuno inflamatorios (recuento de leucocitos, neutrófilos, NLR, SII y proteína C reactiva, etc.) y niveles más bajos de linfocitos y LCR. Además, se observaron niveles más altos de NLR, SII, PLR y un nivel más bajo de LCR en pacientes con ERC que murieron en comparación con los recuperados. En un análisis de la curva de características operativas del receptor, el área NLR, SII, PLR y LCR bajo la curva de mortalidad hospitalaria de pacientes con ERC fueron de 0,830, 0,811, 0,664 y 0,712, respectivamente. Entre todos los parámetros, NLR y SII se dió a conocer la mejor manera de distinguir a los pacientes con mayor riesgo de muerte. Con base en el valor de corte de 1180,5, se encontró que la sensibilidad y especificidad del SII, para predecir la mortalidad hospitalaria, fue del 67,5% y 79,6%, respectivamente. La sensibilidad y especificidad correspondientes del NLR fueron del 85,2% y 66,1%, respectivamente, en el valor de corte de 5,1.
El análisis de regresión logística escalonada hacia adelante mostró que el NLR (≥5,1), SII (≥1180,5) y LCR (≤9) fueron predictores de mortalidad hospitalaria.
Conclusión: Informamos, por primera vez, que el SII es capaz de distinguir pacientes con ERC infectados por COVID-19 de peor supervivencia y, en este sentido, es tan poderoso como el NLR. Como el SII se cuantifica fácilmente a partir de los datos de las muestras de sangre, puede ayudar a la identificación temprana y el manejo oportuno de los pacientes con ERC con peor supervivencia.
Keywords: Chronic kidney disease; Enfermedad renal crónica; Infección por SARS-CoV-2; Mortalidad; Mortality; SARS-CoV-2 infection; Systemic immune inflammation index; Índice de inflamación inmunitaria sistémica.
Copyright © 2021 Sociedad Española de Nefrología. Published by Elsevier España, S.L.U. All rights reserved.
Figures
References
-
- World Health Organization Coronavirus disease (COVID-2019). Situation reports, WHO COVID-19 Dashboard. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio... [accessed 19.5.21].
-
- Republic of Turkey ministry COVID 19 information page. Available from: https://covid19.saglik.gov.tr [accessed 19.5.21].
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
