

Distinct pathophysiological characteristics in developing muscle from patients susceptible to malignant hyperthermia
- PMID: 36792386
- PMCID: PMC10308439
- DOI: 10.1016/j.bja.2023.01.008
Distinct pathophysiological characteristics in developing muscle from patients susceptible to malignant hyperthermia
Abstract
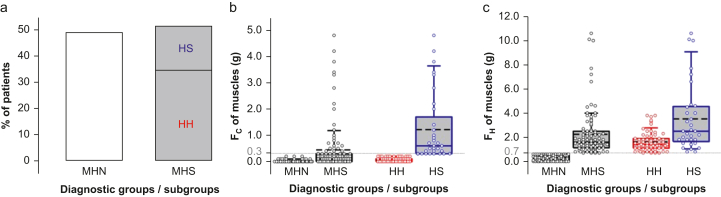
Background: Most patients with malignant hyperthermia susceptibility diagnosed by the in vitro caffeine-halothane contracture test (CHCT) develop excessive force in response to halothane but not caffeine (halothane-hypersensitive). Hallmarks of halothane-hypersensitive patients include high incidence of musculoskeletal symptoms at rest and abnormal calcium events in muscle. By measuring sensitivity to halothane of myotubes and extending clinical observations and cell-level studies to a large group of patients, we reach new insights into the pathological mechanism of malignant hyperthermia susceptibility.
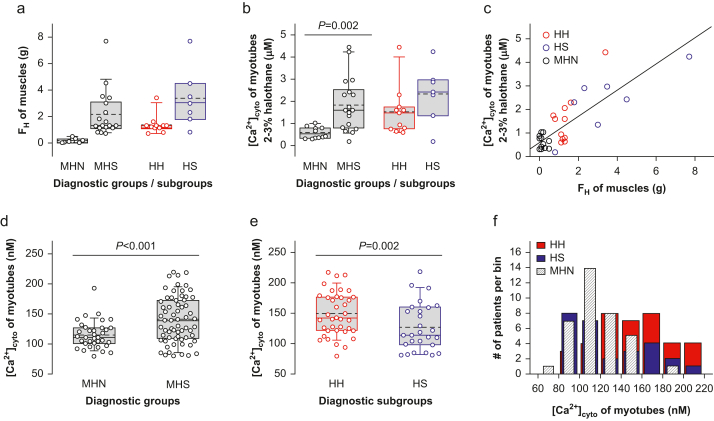
Methods: Patients with malignant hyperthermia susceptibility were classified into subgroups HH and HS (positive to halothane only and positive to both caffeine and halothane). The effects on [Ca2+]cyto of halothane concentrations between 0.5 and 3 % were measured in myotubes and compared with CHCT responses of muscle. A clinical index that summarises patient symptoms was determined for 67 patients, together with a calcium index summarising resting [Ca2+]cyto and spontaneous and electrically evoked Ca2+ events in their primary myotubes.
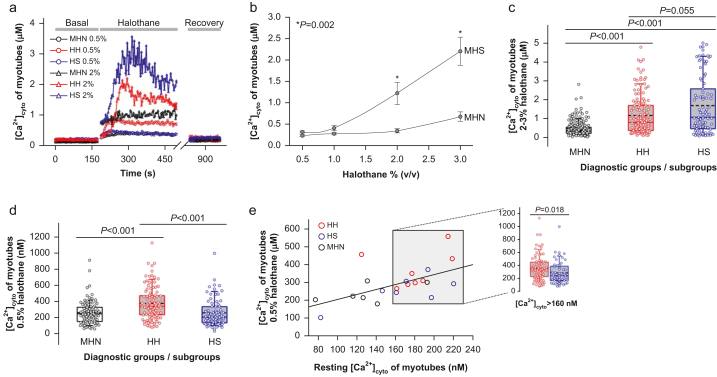
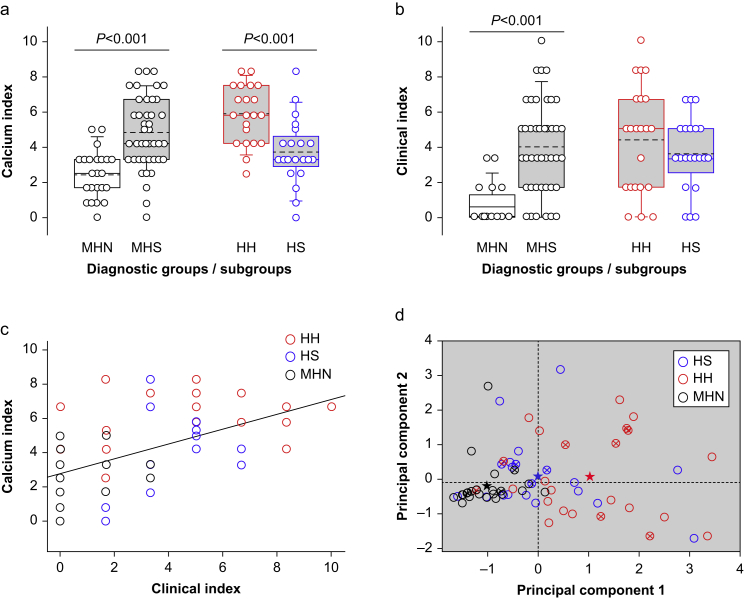
Results: Halothane-hypersensitive myotubes showed a higher response to halothane 0.5% than the caffeine-halothane hypersensitive myotubes (P<0.001), but a lower response to higher concentrations, comparable with that used in the CHCT (P=0.055). The HH group had a higher calcium index (P<0.001), but their clinical index was not significantly elevated vs the HS. Principal component analysis identified electrically evoked Ca2+ spikes and resting [Ca2+]cyto as the strongest variables for separation of subgroups.
Conclusions: Enhanced sensitivity to depolarisation and to halothane appear to be the primary, mutually reinforcing and phenotype-defining defects of halothane-hypersensitive patients with malignant hyperthermia susceptibility.
Keywords: calcium signalling; excitation–contraction coupling; malignant hyperthermia; skeletal muscle; volatile anaesthetics.
Copyright © 2023 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Comment in
-
What is malignant hyperthermia susceptibility?Br J Anaesth. 2023 Jul;131(1):5-8. doi: 10.1016/j.bja.2023.04.014. Epub 2023 May 15. Br J Anaesth. 2023. PMID: 37198032
References
-
- Larach M.G. Standardization of the caffeine halothane muscle contracture test. North American Malignant Hyperthermia Group. Anesth Analg. 1989;69:511–515. - PubMed
-
- Hopkins P.M., Rüffert H., Snoeck M.M., et al. European Malignant Hyperthermia Group guidelines for investigation of malignant hyperthermia susceptibility. Br J Anaesth. 2015;115:531–539. - PubMed
-
- Endo M. Calcium-induced calcium release in skeletal muscle. Physiol Rev. 2009;89:1153–1176. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
