

Learning from the nexus of autoimmunity and cancer
- PMID: 36792572
- PMCID: PMC9986833
- DOI: 10.1016/j.immuni.2023.01.022
Learning from the nexus of autoimmunity and cancer
Abstract
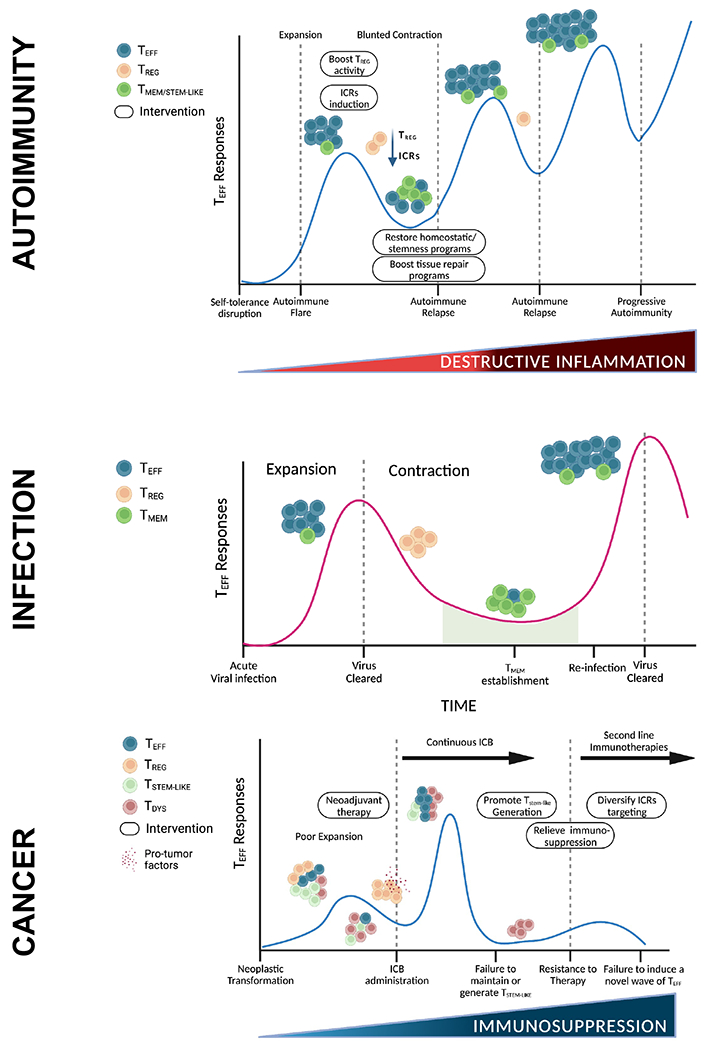
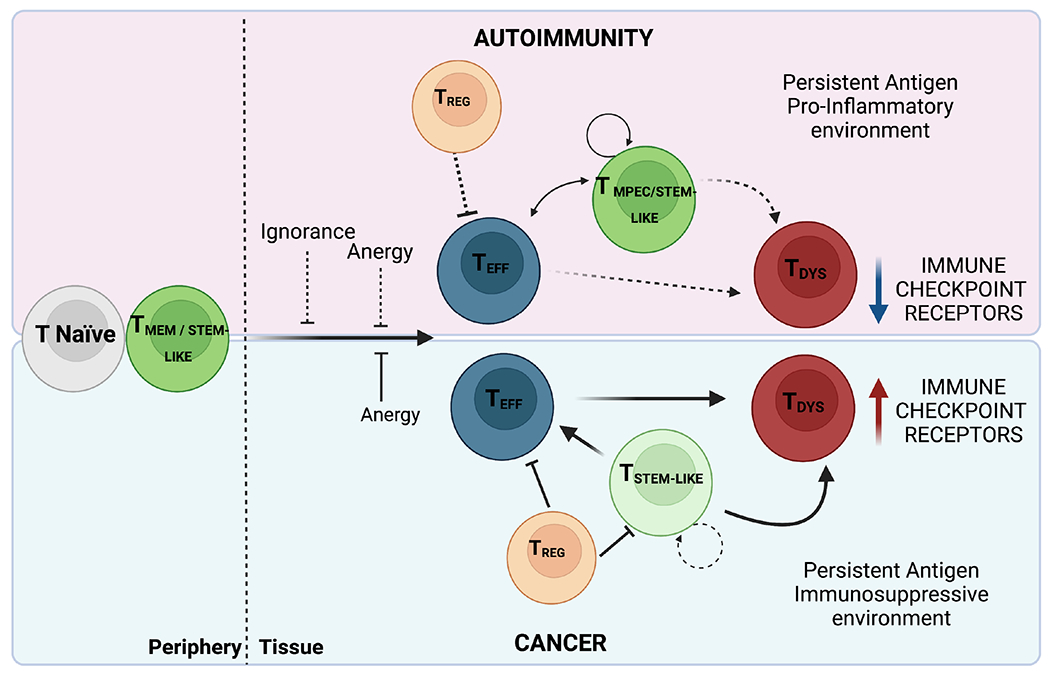
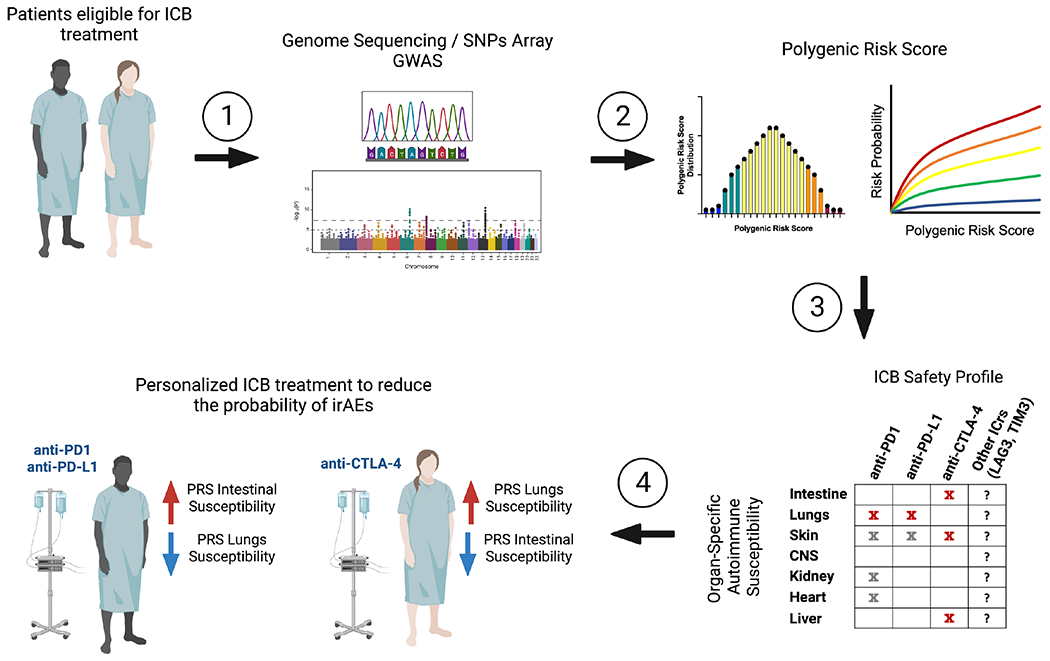
The immune system plays critical roles in both autoimmunity and cancer, diseases at opposite ends of the immune spectrum. Autoimmunity arises from loss of T cell tolerance against self, while in cancer, poor immunity against transformed self fails to control tumor growth. Blockade of pathways that preserve self-tolerance is being leveraged to unleash immunity against many tumors; however, widespread success is hindered by the autoimmune-like toxicities that arise in treated patients. Knowledge gained from the treatment of autoimmunity can be leveraged to treat these toxicities in patients. Further, the understanding of how T cell dysfunction arises in cancer can be leveraged to induce a similar state in autoreactive T cells. Here, we review what is known about the T cell response in autoimmunity and cancer and highlight ways in which we can learn from the nexus of these two diseases to improve the application, efficacy, and management of immunotherapies.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests A.C.A. is a member of the SAB for Tizona Therapeutics, Trishula Therapeutics, Compass Therapeutics, Zumutor Biologics, ImmuneOncia, and Nekonal Sarl. A.C.A. is also a paid consultant for iTeos Therapeutics, Larkspur Biosciences, and Excepgen. A.C.A.’s interests were reviewed and managed by the Brigham and Women’s Hospital and Partners Healthcare in accordance with their conflict-of-interest policies.
Figures
References
-
- Bouneaud C, Kourilsky P, Bousso P. Impact of negative selection on the T cell repertoire reactive to a self-peptide: a large fraction of T cell clones escapes clonal deletion. Immunity. 2000;13(6):829–40. - PubMed
-
- ElTanbouly MA, Noelle RJ. Rethinking peripheral T cell tolerance: checkpoints across a T cell’s journey. Nat Rev Immunol. 2021;21(4):257–67. - PubMed
-
- Hsieh CS, Liang Y, Tyznik AJ, Self SG, Liggitt D, Rudensky AY. Recognition of the peripheral self by naturally arising CD25+ CD4+ T cell receptors. Immunity. 2004;21(2):267–77. - PubMed
-
- Hsieh CS, Zheng Y, Liang Y, Fontenot JD, Rudensky AY. An intersection between the self-reactive regulatory and nonregulatory T cell receptor repertoires. Nat Immunol. 2006;7(4):401–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
