

Cross-municipality migration and spread of tuberculosis in South Africa
- PMID: 36792792
- PMCID: PMC9930008
- DOI: 10.1038/s41598-023-29804-5
Cross-municipality migration and spread of tuberculosis in South Africa
Abstract
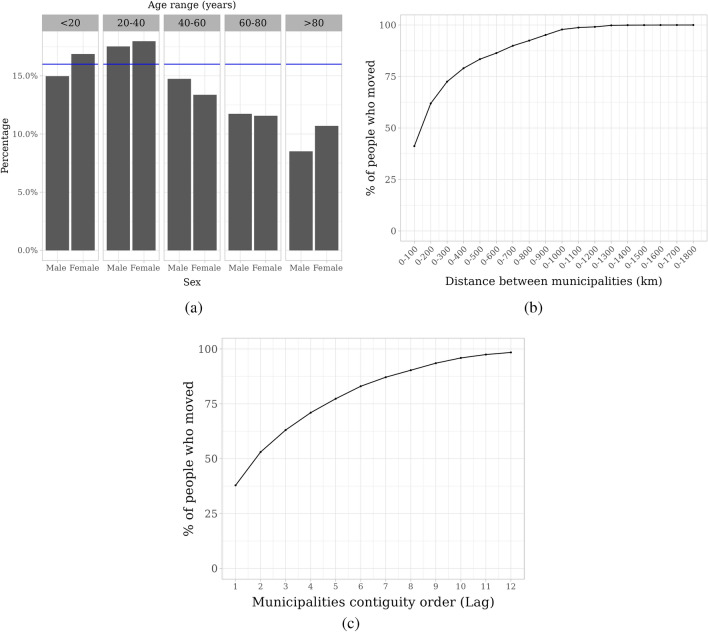
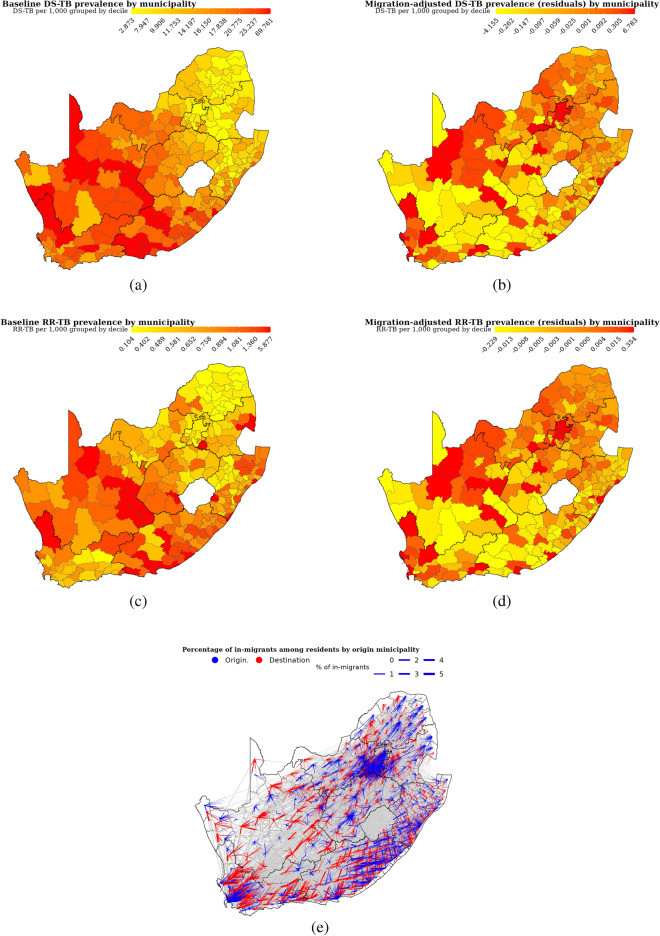
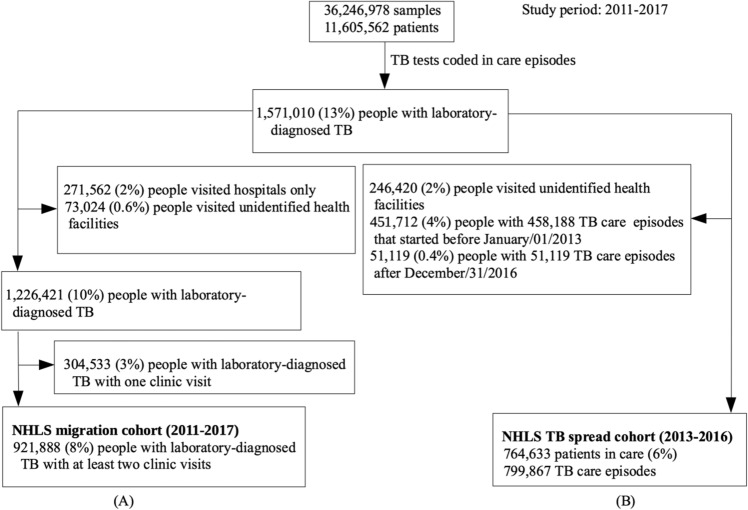
Human migration facilitates the spread of infectious disease. However, little is known about the contribution of migration to the spread of tuberculosis in South Africa. We analyzed longitudinal data on all tuberculosis test results recorded by South Africa's National Health Laboratory Service (NHLS), January 2011-July 2017, alongside municipality-level migration flows estimated from the 2016 South African Community Survey. We first assessed migration patterns in people with laboratory-diagnosed tuberculosis and analyzed demographic predictors. We then quantified the impact of cross-municipality migration on tuberculosis incidence in municipality-level regression models. The NHLS database included 921,888 patients with multiple clinic visits with TB tests. Of these, 147,513 (16%) had tests in different municipalities. The median (IQR) distance travelled was 304 (163 to 536) km. Migration was most common at ages 20-39 years and rates were similar for men and women. In municipality-level regression models, each 1% increase in migration-adjusted tuberculosis prevalence was associated with a 0.47% (95% CI: 0.03% to 0.90%) increase in the incidence of drug-susceptible tuberculosis two years later, even after controlling for baseline prevalence. Similar results were found for rifampicin-resistant tuberculosis. Accounting for migration improved our ability to predict future incidence of tuberculosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
