

The prevalence of left ventricular hypertrophy associated with type-2 diabetes in Shiraz, Iran: a cross-sectional study
- PMID: 36792995
- PMCID: PMC9930283
- DOI: 10.1186/s12872-023-03083-4
The prevalence of left ventricular hypertrophy associated with type-2 diabetes in Shiraz, Iran: a cross-sectional study
Abstract
Background: Left ventricular hypertrophy (LVH) is a common diagnosis in patients with cardiovascular disease (CVD). The prevalence of LVH among patients with Type-2 Diabetes Mellitus (T2DM), high blood pressure and aging is higher than the healthy population and has been independently associated with an increased risk for future cardiac event, including stroke. The aim of this study is to identify the prevalence of LVH among T2DM subjects and evaluate its association with related risk factors of CVD patients in the metropolis of Shiraz, Iran. The novelty of this study is that there has been no known published epidemiological study related to the relationship of LVH and T2DM on this unique population.
Materials and method: This cross-sectional study was designed based on collected data of 7715 free dwelling subjects in the community-based Shiraz Cohort Heart Study (SCHS) from 2015 to 2021, ages 40-70 years. Overall, 1118 subjects with T2DM were identified in the SCHS and after exclusion criteria, 595 subjects remained eligible for study. Subjects with electrocardiography (ECG) results, which are appropriate and diagnostics tools, were evaluated for the presence of LVH. Thus, the variables related to LVH and non-LVH in subjects with diabetes were analyzed using version-22 statistical package for social sciences software program to ensure consistency, accuracy, reliability, and validity for final analysis. Based upon related variables and identifying LVH and non-LVH subjects, the relevant statistical analysis was implemented to ensure its consistency, accuracy, reliability, and validity for final analysis.
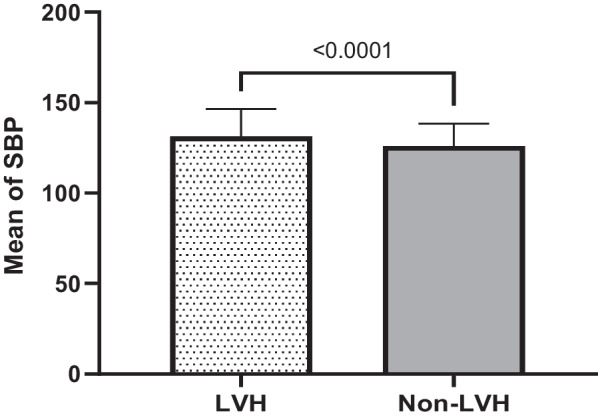
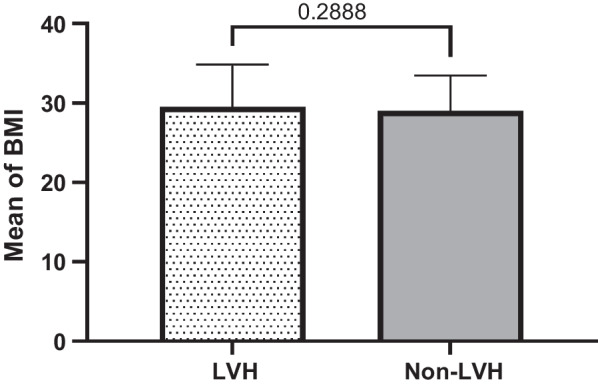
Results: Overall, the prevalence of diabetic subjects was 14.5% in the SCHS study. Furthermore, the prevalence of hypertension in the study subjects aged 40-70 years was 37.8%. The prevalence of hypertension history in T2DM study subjects for LVH compared to non-LVH was (53.7% vs. 33.7%). The prevalence of LVH among patients with T2DM as the primary target of this study was 20.7%. Analytical findings comparing both LVH and non-LVH subjects who have T2DM identified significance for variables in the older (≥ 60) mean and categorical age group (P < 0.0001), history of hypertension (P < 0.0001), mean and categorical duration of hypertension in years (P < 0.0160), status of controlled versus uncontrolled hypertension level (P < 0.0120), the mean systolic blood pressure (P < 0.0001) as well as mean duration years of T2DM and categorical duration of diabetes in years (< 0.0001 and P < 0.0060), mean fasting blood sugar (< 0.0307) and categorical status of FBS Level (mg/dl): controlled and uncontrolled FBS status of controlled vs. uncontrolled FBS levels P < 0.0020). However, there were no significant findings for gender (P = 0.3112), diastolic blood pressure mean (P = 0.7722) and body mass index (BMI) mean and categorical BMI (P = 0.2888 and P = 0.4080, respectively).
Conclusion: The prevalence of LVH in the study increases significantly among T2DM patients with hypertension, older age, years of hypertension, years of diabetes, and higher FBS. Thus, given the significant risk of diabetes and CVD, evaluation of LVH through reasonable diagnostic testing with ECG can help reduce the risk of future complications through the development of risk factor modifications and treatments guidelines.
Keywords: CVD; ECG; LVH; T2DM.
© 2023. The Author(s).
Conflict of interest statement
None declared.
Figures





References
-
- Soteriades ES, Targino MC, Talias MA, Hauser R, Kawachi I, Christiani DC, et al. Obesity and risk of LVH and ECG abnormalities in US firefighters. J Occup Environ Med. 2011;53(8):867–871. - PubMed
-
- Wang SX, Xue H, Zou YB, Sun K, Fu CY, Wang H, et al. Prevalence and risk factors for left ventricular hypertrophy and left ventricular geometric abnormality in the patients with hypertension among Han Chinese. Chin Med J (Engl) 2012;125(1):21–26. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
