

Parent artery occlusion for ruptured aneurysms in moyamoya vessels or on collaterals
- PMID: 36793491
- PMCID: PMC9923357
- DOI: 10.3389/fneur.2023.1085120
Parent artery occlusion for ruptured aneurysms in moyamoya vessels or on collaterals
Abstract
Background: Aneurysms in moyamoya vessels or on collaterals are difficult to treat. Parent artery occlusion (PAO) via endovascular treatment (EVT) is often the last resort, but the safety and efficacy of this approach need to be evaluated.
Materials and methods: A retrospective study was performed on patients admitted to our hospital who were diagnosed with unilateral or bilateral moyamoya disease (MMD) associated with ruptured aneurysms in moyamoya vessels or on collaterals. These aneurysms were treated with PAO, and the clinical outcome was recorded.
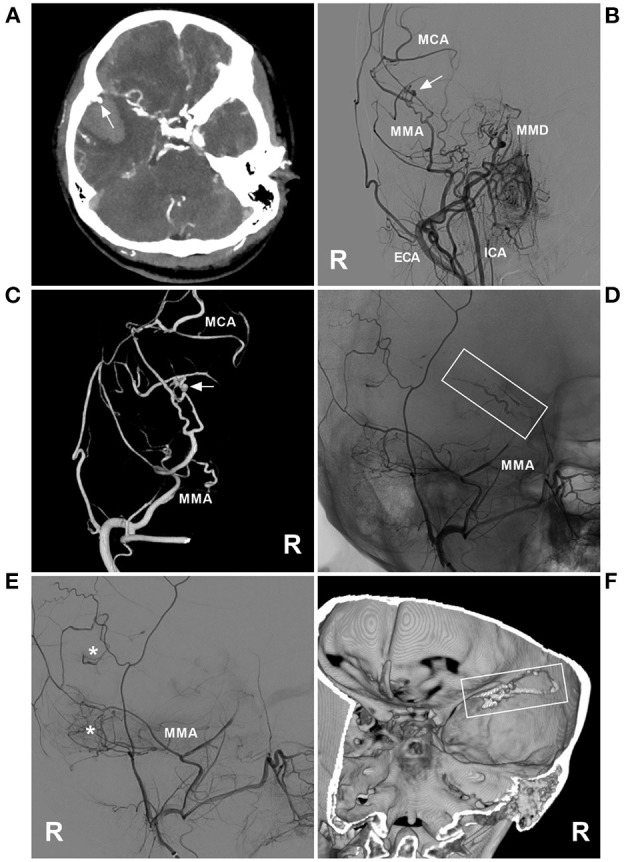
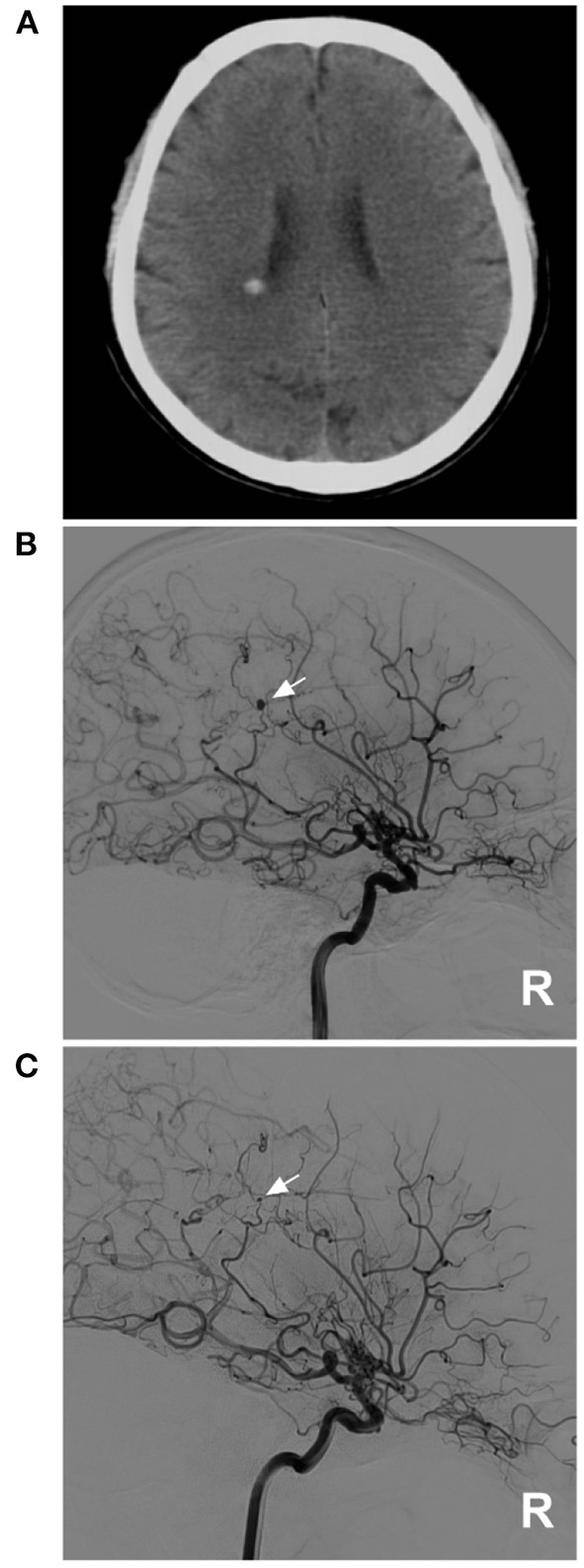
Results: Eleven patients were aged 54.7 ± 10.4 years, and six patients were male (54.5%, 6/11). The aneurysms in 11 patients were single and ruptured, and the average size was 2.7 ± 0.6 mm. Three (27.3%, 3/11) aneurysms were located at the distal anterior choroidal artery, 3 (27.3%, 3/11) were at the distal lenticulostriate artery, 3 (27.3%, 3/11) were at the P2-3 segment of the posterior cerebral artery, 1 (9.1%, 1/11) was at the P4-5 segment of the posterior cerebral artery, and 1 was at the transdural location of the middle meningeal artery. Among the 11 aneurysms, PAO by coiling was performed on 7 (63.6%, 7/11), and Onyx casting was performed on 4 (36.4%, 4/11). Of 11 patients, 2 (18.2%, 2/11) suffered intraoperative hemorrhagic complications. During follow-up, all patients had good outcomes with a modified Rankin scale score of 0-2.
Conclusion: As a last resort, the application of PAO with coiling or casting Onyx for ruptured aneurysms in moyamoya vessels or on collaterals may be safe with an acceptable clinical outcome. However, patients with MMD may not always achieve expected health outcomes, and PAO for the aneurysm can bring only temporary relief.
Keywords: aneurysm; collateral; moyamoya disease; outcome; parent artery occlusion.
Copyright © 2023 Zhou, Xu and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Fetal-type posterior cerebral artery: the pitfall of parent artery occlusion for ruptured P₂ segment and distal aneurysms.J Neurosurg. 2015 Oct;123(4):906-14. doi: 10.3171/2014.9.JNS1442. Epub 2015 Mar 13. J Neurosurg. 2015. PMID: 25768832
-
Treatment of aneurysms in patients with moyamoya disease: a 10-year single-center experience.J Neurosurg. 2018 Jun;128(6):1813-1822. doi: 10.3171/2017.3.JNS162290. Epub 2017 Aug 25. J Neurosurg. 2018. PMID: 28841118
-
The prospects and pitfalls in the endovascular treatment of moyamoya disease-associated intracranial aneurysms.Neurosurg Rev. 2021 Feb;44(1):261-271. doi: 10.1007/s10143-020-01261-y. Epub 2020 Feb 12. Neurosurg Rev. 2021. PMID: 32052219 Review.
-
Parent artery occlusion with Onyx for distal aneurysms of posterior inferior cerebellar artery: a single-centre experience in a series of 15 patients.Neurol India. 2013 May-Jun;61(3):265-9. doi: 10.4103/0028-3886.115066. Neurol India. 2013. PMID: 23860146
-
Endovascular Treatment of Posterior Cerebral Artery Trunk Aneurysm: The Status Quo and Dilemma.Front Neurol. 2022 Jan 6;12:746525. doi: 10.3389/fneur.2021.746525. eCollection 2021. Front Neurol. 2022. PMID: 35069405 Free PMC article. Review.
Cited by
-
Spontaneous Middle Meningeal Artery Aneurysms: A Case Report and Review of the Literature.Cureus. 2023 Nov 25;15(11):e49407. doi: 10.7759/cureus.49407. eCollection 2023 Nov. Cureus. 2023. PMID: 38149141 Free PMC article.
-
Aneurysmal formation of periventricular anastomosis is associated with collateral development of Moyamoya disease and its rupture portends poor prognosis: detailed analysis by multivariate statistical and machine learning approaches.Neurosurg Rev. 2024 Nov 19;47(1):856. doi: 10.1007/s10143-024-03097-2. Neurosurg Rev. 2024. PMID: 39557727 Free PMC article.
References
-
- Suzuki J, Kodama N. Moyamoya disease: a review. Stroke. (1983) 14:104–9. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials