

Locoregional treatment of de novo stage IV breast cancer in the era of modern oncology
- PMID: 36793604
- PMCID: PMC9923000
- DOI: 10.3389/fonc.2023.1083297
Locoregional treatment of de novo stage IV breast cancer in the era of modern oncology
Abstract
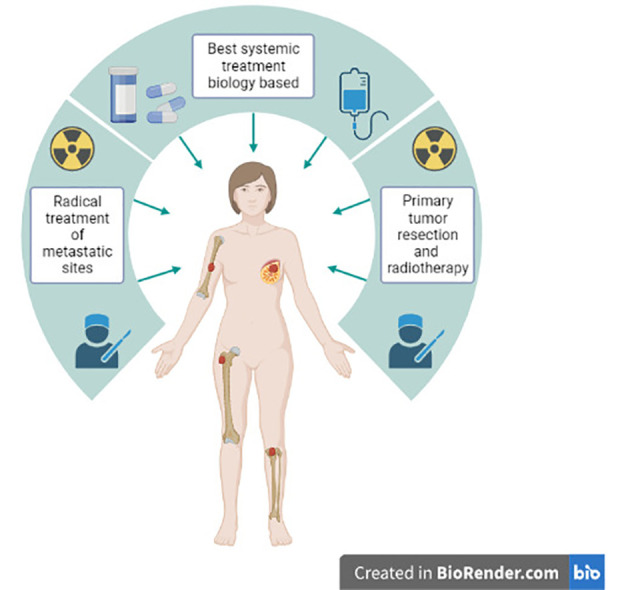
Approximately 6% of metastatic breast cancers arise de novo. While systemic therapy (ST) remains the treatment backbone as for patients with metachronous metastases, locoregional treatment (LRT) of the primary tumor remains a controversial method. The removal of the primary has an established role for palliative purposes, but it is unclear if it could also determine a survival benefit. Retrospective evidence and pre-clinical studies seem to support the removal of the primary as an effective approach to improve survival. On the other hand, most randomized evidence suggests avoiding LRT. Both retrospective and prospective studies suffer several limitations, ranging from selection bias and outdated ST to a small sample of patients. In this review we discuss available data and try to identify subgroups of patients which could benefit the most from LRT of the primary, to facilitate clinical practice decisions, and to hypothesize future studies design on this topic.
Keywords: breast cancer; locoregional treatment; primary tumor; radiotherapy; stage IV; surgery.
Copyright © 2023 Merloni, Palleschi, Gianni, Casadei, Curcio, Romeo, Rocchi, Cima, Sirico, Sarti, Cecconetto, Mariotti, Di Menna and De Giorgi.
Conflict of interest statement
UD received honoraria for advisory boards or speaker fees for Pfizer, BMS, MSD, PharmaMar, Astellas, Bayer, Ipsen, Roche, Novartis, Clovis, GSK, AstraZeneca, Institutional research grants from AstraZeneca, Sanofi and Roche. MP has received advisory board fees from Novartis. All other authors confirm that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources