

Predicting the survival benefit of liver transplantation in HBV-related acute-on-chronic liver failure: an observational cohort study
- PMID: 36793753
- PMCID: PMC9923183
- DOI: 10.1016/j.lanwpc.2022.100638
Predicting the survival benefit of liver transplantation in HBV-related acute-on-chronic liver failure: an observational cohort study
Abstract
Background: Liver transplantation (LT) is an effective therapy for acute-on-chronic liver failure (ACLF) but is limited by organ shortages. We aimed to identify an appropriate score for predicting the survival benefit of LT in HBV-related ACLF patients.
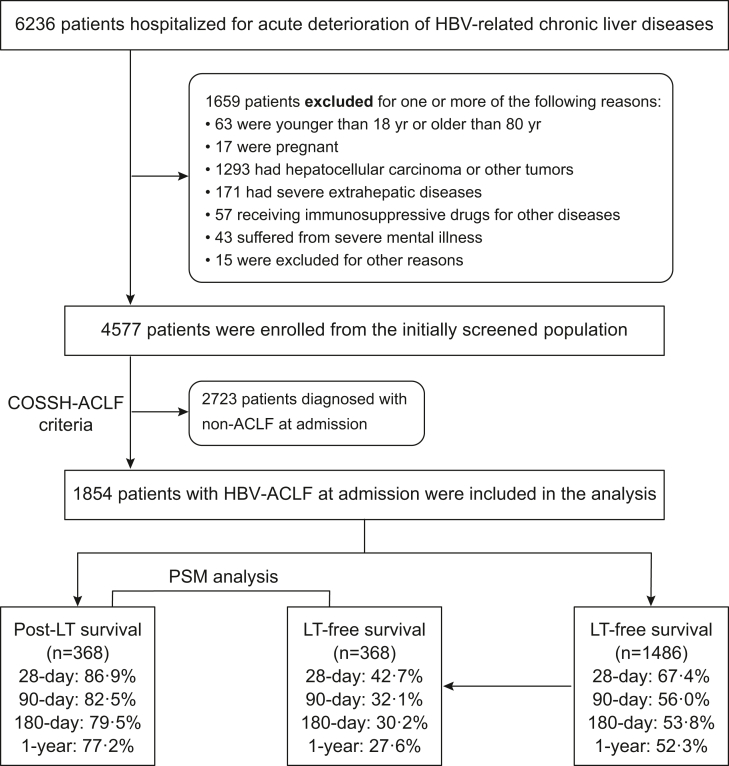
Methods: Hospitalized patients with acute deterioration of HBV-related chronic liver disease (n = 4577) from the Chinese Group on the Study of Severe Hepatitis B (COSSH) open cohort were enrolled to evaluate the performance of five commonly used scores for predicting the prognosis and transplant survival benefit. The survival benefit rate was calculated to reflect the extended rate of the expected lifetime with vs. without LT.
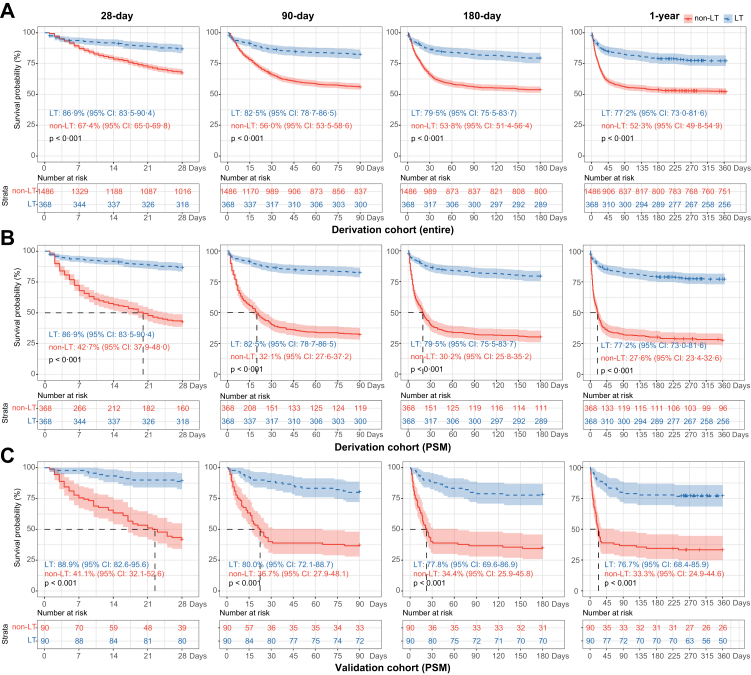
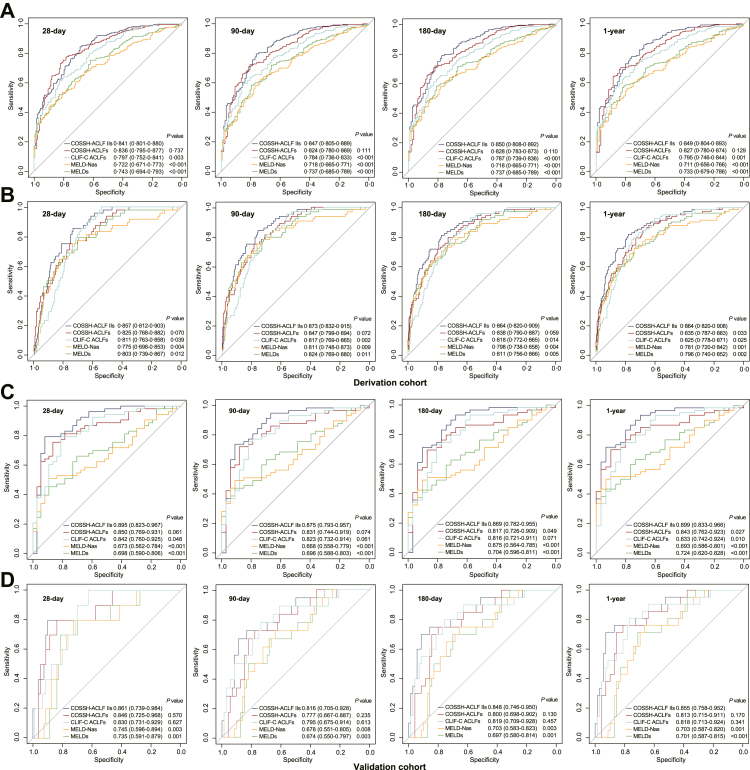
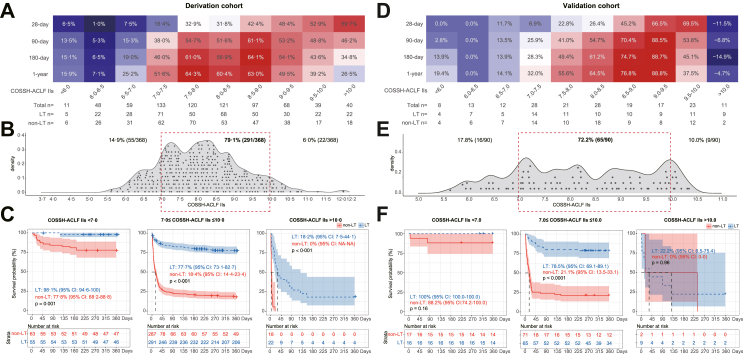
Findings: In total, 368 HBV-ACLF patients received LT. They showed significantly higher 1-year survival than those on the waitlist in both the entire HBV-ACLF cohort (77.2%/52.3%, p < 0.001) and the propensity score matching cohort (77.2%/27.6%, p < 0.001). The area under the receiver operating characteristic curve (AUROC) showed that the COSSH-ACLF II score performed best (AUROC 0.849) at identifying the 1-year risk of death on the waitlist and best (AUROC 0.864) at predicting 1-year outcome post-LT (COSSH-ACLFs/CLIF-C ACLFs/MELDs/MELD-Nas: AUROC 0.835/0.825/0.796/0.781; all p < 0.05). The C-indexes confirmed the high predictive value of COSSH-ACLF IIs. Survival benefit rate analyses showed that patients with COSSH-ACLF IIs 7-10 had a higher 1-year survival benefit rate from LT (39.2%-64.3%) than those with score <7 or >10. These results were prospectively validated.
Interpretation: COSSH-ACLF IIs identified the risk of death on the waitlist and accurately predicted post-LT mortality and survival benefit for HBV-ACLF. Patients with COSSH-ACLF IIs 7-10 derived a higher net survival benefit from LT.
Funding: This study was supported by the National Natural Science Foundation of China (No. 81830073, No. 81771196) and the National Special Support Program for High-Level Personnel Recruitment (Ten-thousand Talents Program).
Keywords: ACLF, acute-on-chronic liver failure; AUROC, area under the receiver operating characteristic curve; Acute-on-chronic liver failure; CLIF-C ACLFs, CLIF-C ACLF score; CLIF-C, chronic liver failure Consortium; CLIF-OFs, CLIF-organ failure score; COSSH, Chinese Group on the Study of Severe Hepatitis B; COSSH-ACLF IIs, COSSH-ACLF II score; COSSH-ACLFs, COSSH-ACLF score; EASL, European Association for the Study of the Liver; HBV, hepatitis B virus; HE, hepatic encephalopathy; Hepatitis B virus; INR, international normalized ratio; LT, liver transplantation; Liver transplantation; MELD-Nas, MELD-sodium score; MELDs, Model for End-stage Liver Disease score; PSM, propensity score matching; Survival benefit; TB, total bilirubin; Transplant timing.
© 2022 The Author(s).
Conflict of interest statement
None of the authors have competing interests to declare.
Figures
References
-
- Iannacone M., Guidotti L.G. Immunobiology and pathogenesis of hepatitis B virus infection. Nat Rev Immunol. 2022;22:19–32. - PubMed
-
- Global hepatitis report 2017. World Health Organization; Geneva: 2017.
-
- Wu T., Li J., Shao L., et al. Development of diagnostic criteria and a prognostic score for hepatitis B virus-related acute-on-chronic liver failure. Gut. 2018;67:2181–2191. - PubMed
-
- Arroyo V., Moreau R., Jalan R. Acute-on-chronic liver failure. N Engl J Med. 2020;382:2137–2145. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
