

Robotic locomotor training for spasticity, pain, and quality of life in individuals with chronic SCI: A pilot randomized controlled trial
- PMID: 36793803
- PMCID: PMC9922844
- DOI: 10.3389/fresc.2023.1003360
Robotic locomotor training for spasticity, pain, and quality of life in individuals with chronic SCI: A pilot randomized controlled trial
Abstract
Objective: The prevention and treatment of secondary complications is a key priority for people with spinal cord injury and a fundamental goal of rehabilitation. Activity-based Training (ABT) and Robotic Locomotor Training (RLT) demonstrate promising results for reducing secondary complications associated with SCI. However, there is a need for increased evidence through randomized controlled trials. Therefore, we aimed to investigate the effect of RLT and ABT interventions on pain, spasticity, and quality of life in individuals with spinal cord injuries.
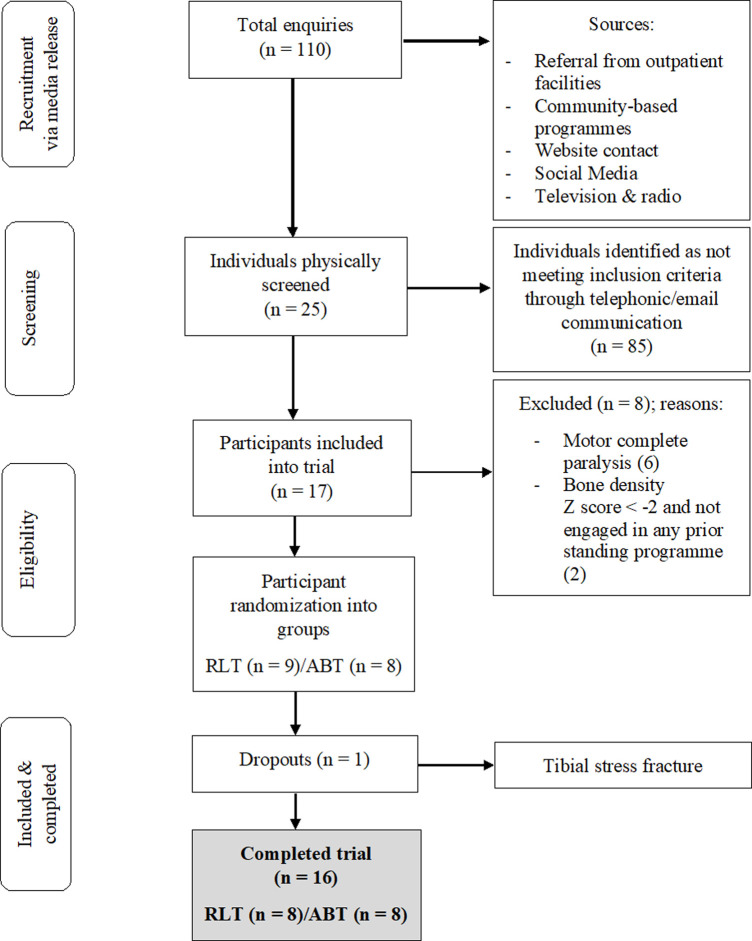
Methods: Participants with chronic motor incomplete tetraplegia (n = 16) were recruited. Each intervention involved 60-minute sessions, 3× per week, over 24-weeks. RLT involved walking in an Ekso GT exoskeleton. ABT involved a combination of resistance, cardiovascular and weight-bearing exercise. Outcomes of interest included the Modified Ashworth Scale, the International SCI Pain Basic Data Set Version 2, and the International SCI Quality of Life Basic Data Set.
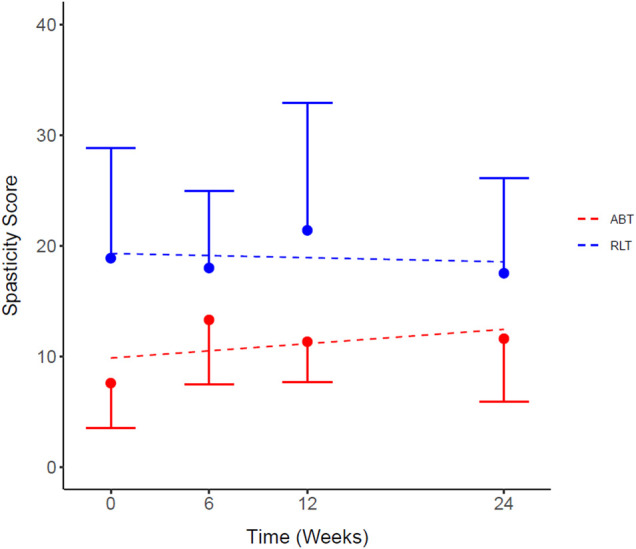
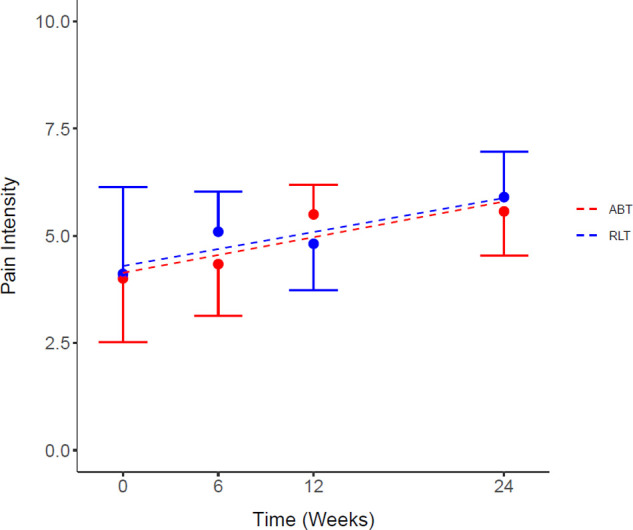
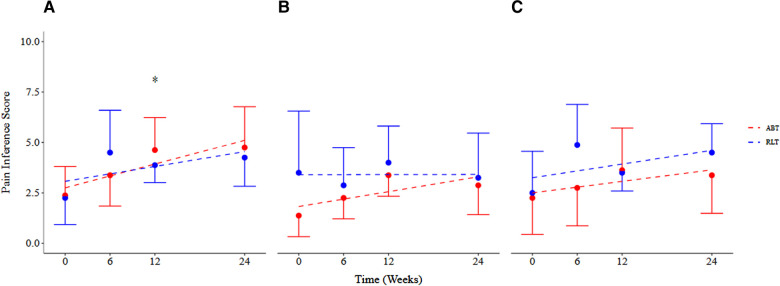
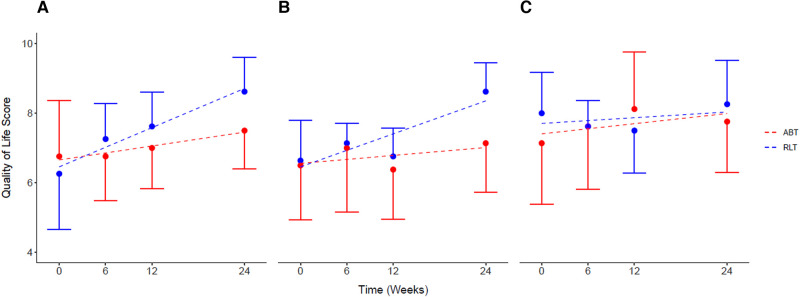
Results: Neither intervention altered symptoms of spasticity. Pain intensity increased from pre-post intervention for both groups, with a mean increase of 1.55 [-0.82, 3.92] (p = 0.03) and 1.56 [-0.43, 3.55] (p = 0.02) points for the RLT and ABT group, respectively. The ABT group had an increase in pain interference scores of 100%, 50%, and 109% for the daily activity, mood, and sleep domain, respectively. The RLT group had an increase in pain interference scores of 86% and 69% for the daily activity and mood domain respectively, but no change in the sleep domain. The RLT group had increased perceptions of quality of life with changes of 2.37 [0.32, 4.41], 2.00 [0.43, 3.56] and 0.25 [-1.63, 2.13] points, p = 0.03, for the general, physical, and psychological domains, respectively. The ABT group had increased perceptions of general, physical and psychological quality of life with changes of 0.75 [-1.38, 2.88], 0.62 [-1.83, 3.07] and 0.63 [-1.87, 3.13] points, respectively.
Conclusions: Despite increased pain ratings and no change in symptoms of spasticity, there was an increase in perceived quality of life for both groups over 24-weeks. This dichotomy warrants additional investigation in future large-scale randomized controlled trials.
Keywords: exercise therapy; exoskeleton device; muscle spasticity; pain; quality of life; spinal cord injuries.
© 2023 Shackleton, Evans, West, Derman and Albertus.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Robotic Locomotor Training Leads to Cardiovascular Changes in Individuals With Incomplete Spinal Cord Injury Over a 24-Week Rehabilitation Period: A Randomized Controlled Pilot Study.Arch Phys Med Rehabil. 2021 Aug;102(8):1447-1456. doi: 10.1016/j.apmr.2021.03.018. Epub 2021 Apr 9. Arch Phys Med Rehabil. 2021. PMID: 33839105 Clinical Trial.
-
Robotic locomotor training in a low-resource setting: a randomized pilot and feasibility trial.Disabil Rehabil. 2024 Jul;46(15):3363-3372. doi: 10.1080/09638288.2023.2245751. Epub 2023 Aug 22. Disabil Rehabil. 2024. PMID: 37605978 Clinical Trial.
-
Foundational ingredients of robotic gait training for people with incomplete spinal cord injury during inpatient rehabilitation (FIRST): A randomized controlled trial protocol.PLoS One. 2022 May 10;17(5):e0267013. doi: 10.1371/journal.pone.0267013. eCollection 2022. PLoS One. 2022. PMID: 35536844 Free PMC article.
-
Effectiveness of over-ground robotic locomotor training in improving walking performance, cardiovascular demands, secondary complications and user-satisfaction in individuals with spinal cord injuries: A systematic review.J Rehabil Med. 2019 Oct 29;51(10):723-733. doi: 10.2340/16501977-2601. J Rehabil Med. 2019. PMID: 31511902
-
Effects of Robot-Assisted Gait Training in Individuals with Spinal Cord Injury: A Meta-analysis.Biomed Res Int. 2020 Mar 21;2020:2102785. doi: 10.1155/2020/2102785. eCollection 2020. Biomed Res Int. 2020. PMID: 32280681 Free PMC article. Review.
Cited by
-
Quantifying Treatments as Usual and with Technologies in Neurorehabilitation of Individuals with Spinal Cord Injury.Healthcare (Basel). 2024 Sep 13;12(18):1840. doi: 10.3390/healthcare12181840. Healthcare (Basel). 2024. PMID: 39337181 Free PMC article.
-
Epidural Stimulation and Resistance Training (REST-SCI) for Overground Locomotion After Spinal Cord Injury: Randomized Clinical Trial Protocol.J Clin Med. 2025 Mar 8;14(6):1829. doi: 10.3390/jcm14061829. J Clin Med. 2025. PMID: 40142643 Free PMC article.
-
Cryoneurolysis and Quadriplegia: A Case Report on Pain and Severe Spasticity Management.Arch Rehabil Res Clin Transl. 2024 Oct 5;6(4):100374. doi: 10.1016/j.arrct.2024.100374. eCollection 2024 Dec. Arch Rehabil Res Clin Transl. 2024. PMID: 39822204 Free PMC article.
References
-
- Ginis KAM, Latimer AE, Mckechnie K, Ditor DS, Mccartney N, Hicks AL, et al. Using exercise to enhance subjective well-being among people with spinal cord injury: the mediating influences of stress and pain. Rehabil Psychol. (2003) 48(3):157–64. 10.1037/0090-5550.48.3.157 - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous