

Uniportal fully robotic-assisted sleeve resections: surgical technique and initial experience of 30 cases
- PMID: 36793981
- PMCID: PMC9922765
- DOI: 10.21037/acs-2022-urats-23
Uniportal fully robotic-assisted sleeve resections: surgical technique and initial experience of 30 cases
Abstract
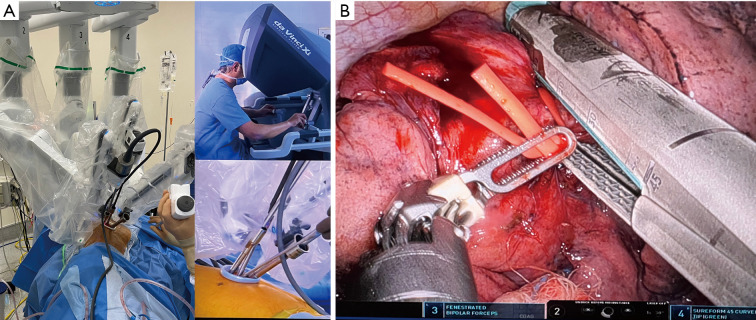
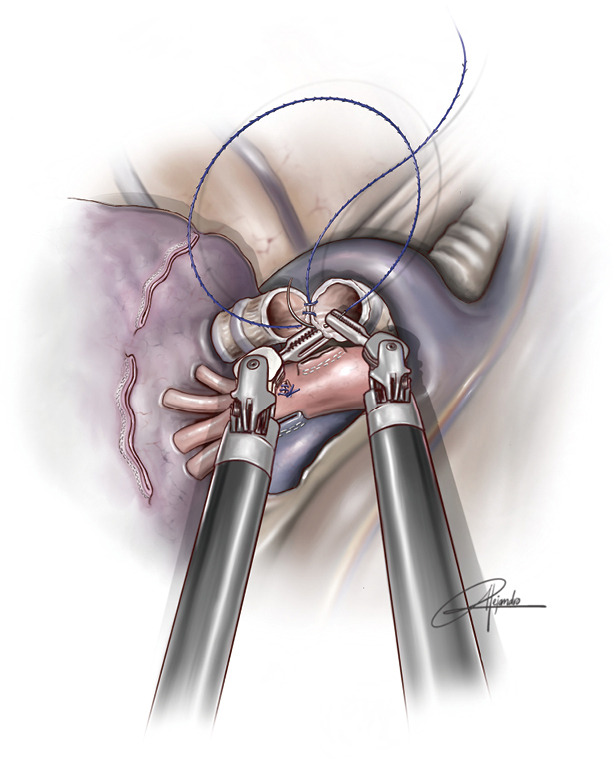
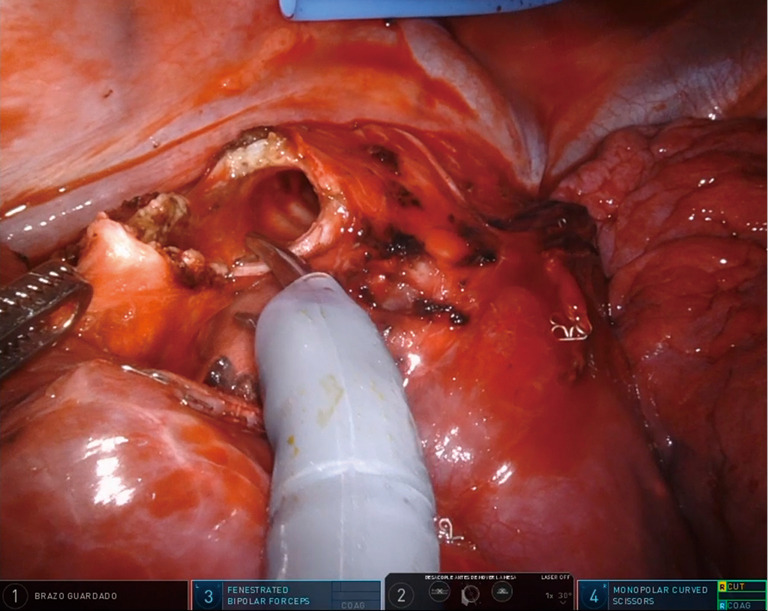
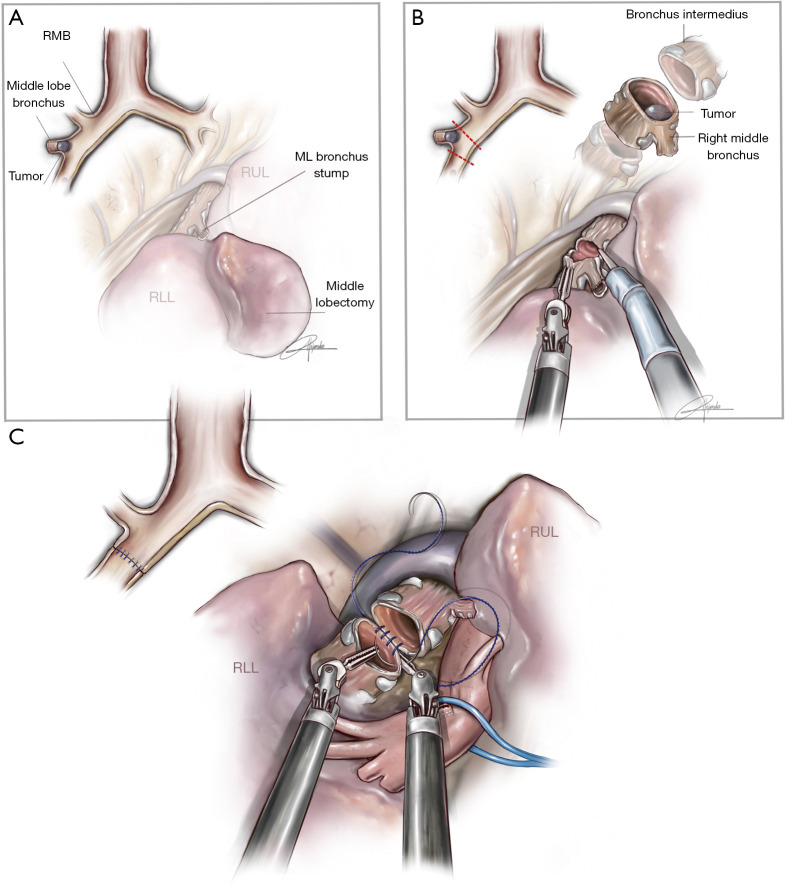
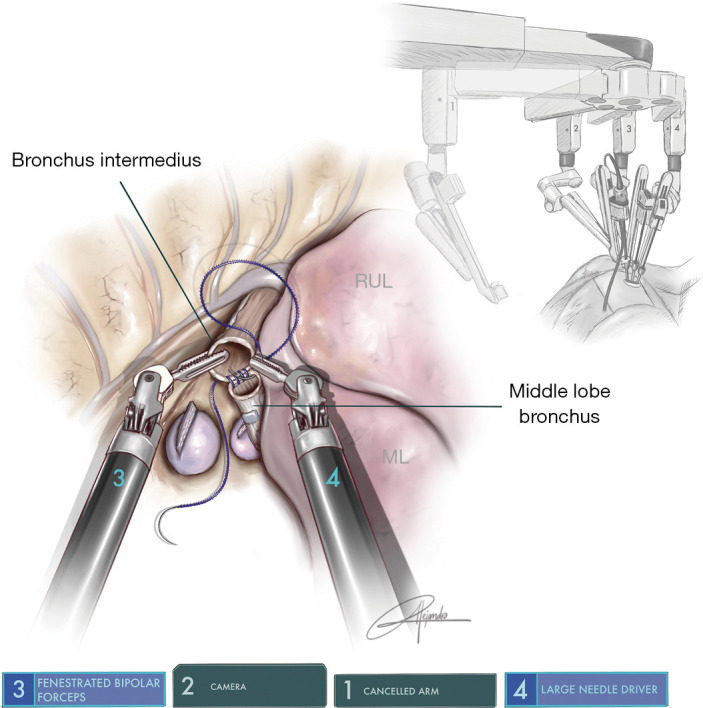
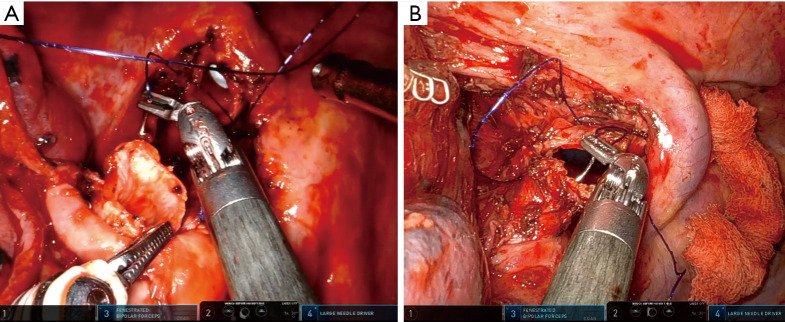
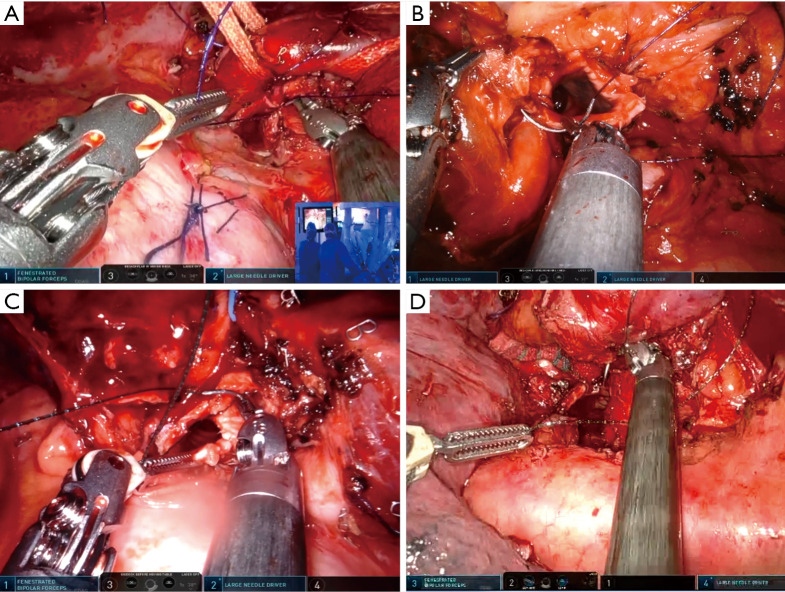
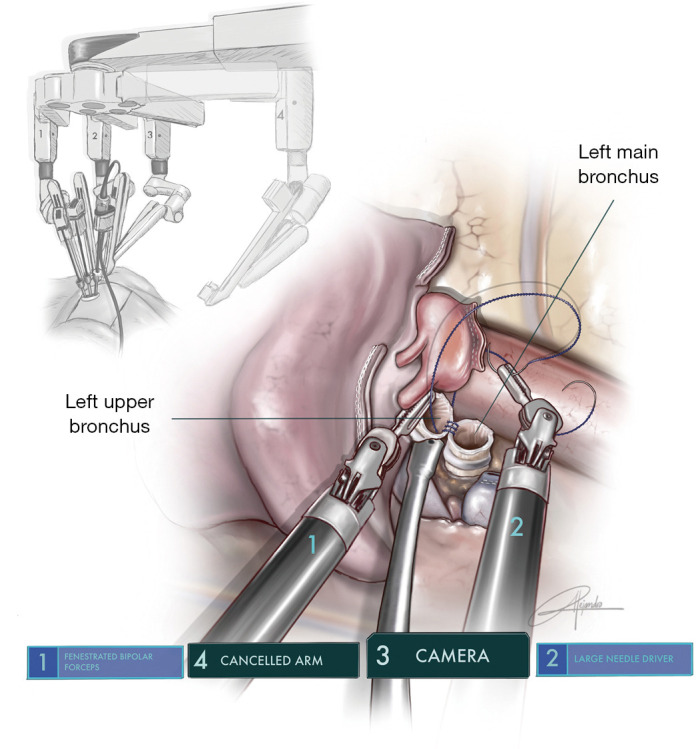
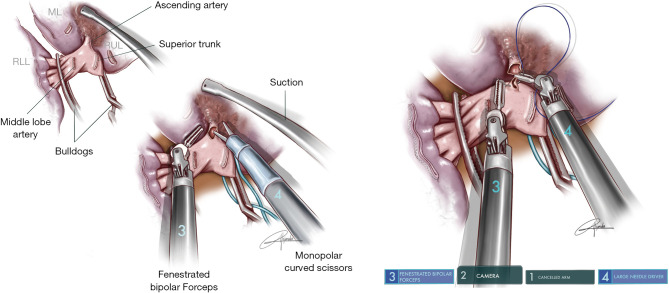
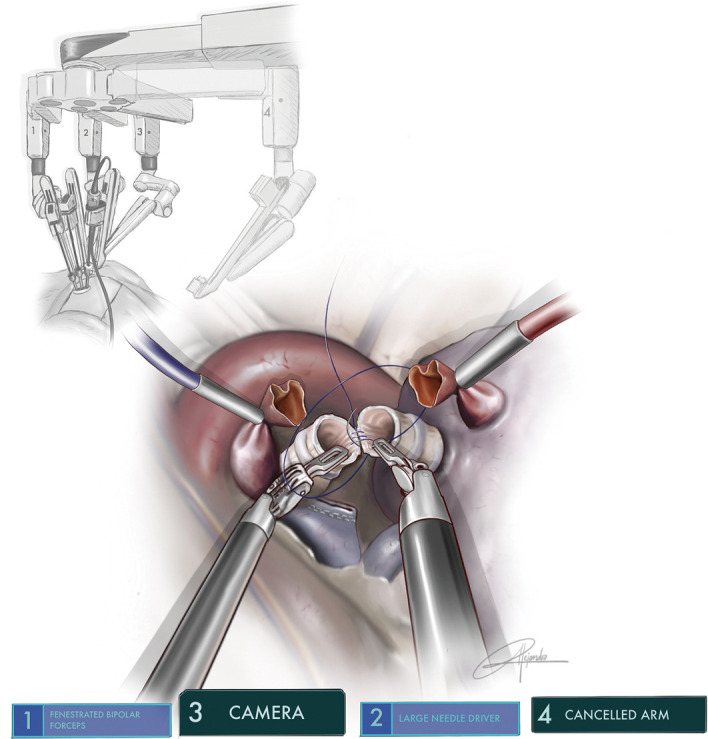
Since the first uniportal video-assisted thoracoscopic surgery (uVATS) performed in 2010, the uniportal approach has evolved up to a point where even the most complex cases can be done. This is thanks to the experience acquired over the years, the specifically designed instruments and improvements in imaging. However, in these last few years, robotic-assisted thoracoscopic surgery (RATS) has also shown progress and distinct advantages compared to the uniportal VATS approach, thanks to advanced maneuverability of the robotic arms as well as the three-dimensional (3D) view. Excellent surgical outcomes have been reported and so too, the ergonomic benefits to the surgeon. The main limitation we find of the robotic systems is that they are designed for a multiport approach, requiring between three to five incisions to be able to perform surgeries. With the aim to offer the least invasive approach, using the robotic technology we decided to adapt the Da Vinci Xi® in September 2021 to develop the uniportal pure RATS approach (uRATS) performed by a single intercostal incision, without rib spreading and using the robotic staplers. We have now reached a point where we perform all type of procedures, including the more complex sleeve resections. Sleeve lobectomy is now widely accepted as a reliable and safe procedure to allow complete resection of centrally located tumors. Although it is a technically challenging surgical technique, it offers better outcomes when compared to pneumonectomy. The intrinsic characteristics of the robot such as the 3D view and improved maneuverability of instruments make the sleeve resections easier compared to thoracoscopic techniques. As in uVATS vs. multiport VATS, the uRATS approach, due to its geometrical characteristics, requires specific instrumentation, different movements and learning curve compared to multiport RATS. In this article we describe the surgical technique and our initial uniportal pure RATS experience with bronchial, vascular sleeves and carinal resections in 30 patients.
Keywords: Sleeve lobectomy; lung cancer; uRATS sleeve; uniportal robotic-assisted thoracoscopic surgery (uRATS).
2023 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Oh DS, Cho I, Karamian B, et al. Early adoption of robotic pulmonary lobectomy: feasibility and initial outcomes. Am Surg 2013;79:1075-80. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials