

Carbapenem-resistant gram-negative bacterial infection in intensive care unit patients: Antibiotic resistance analysis and predictive model development
- PMID: 36794004
- PMCID: PMC9922834
- DOI: 10.3389/fcimb.2023.1109418
Carbapenem-resistant gram-negative bacterial infection in intensive care unit patients: Antibiotic resistance analysis and predictive model development
Abstract
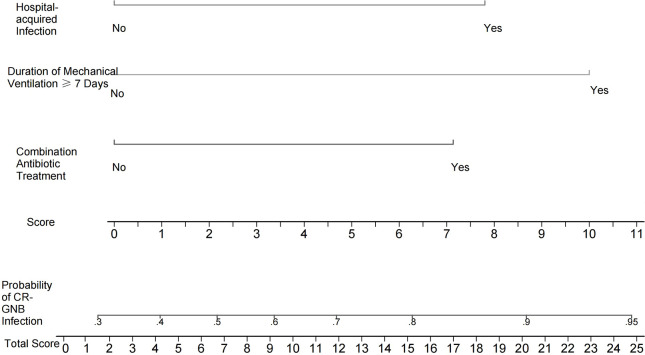
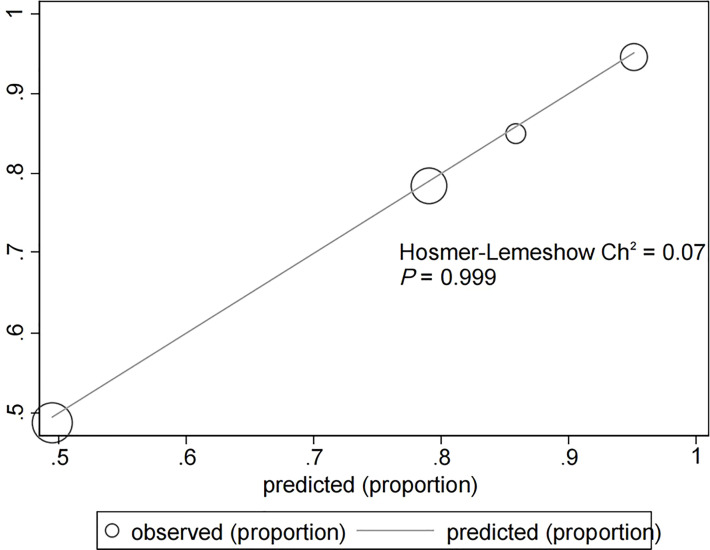
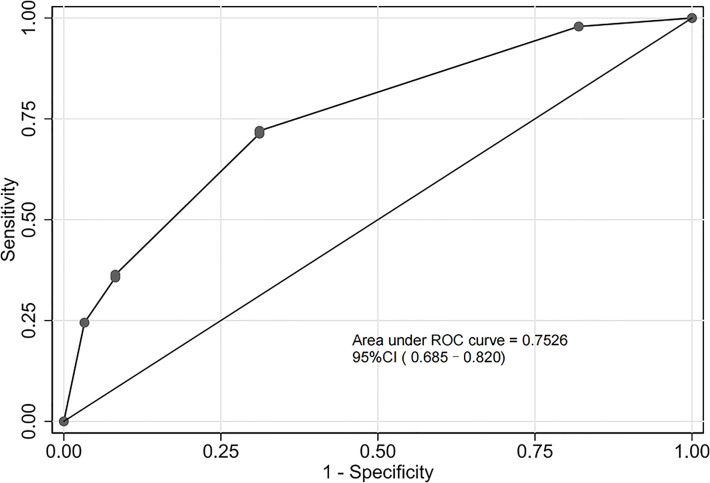
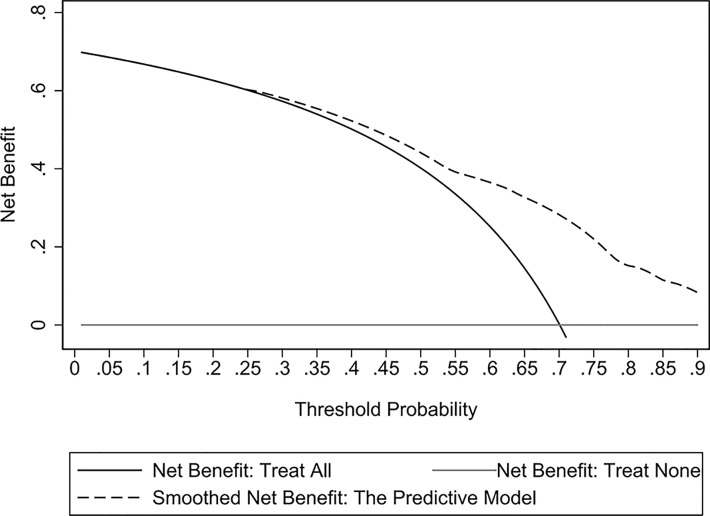
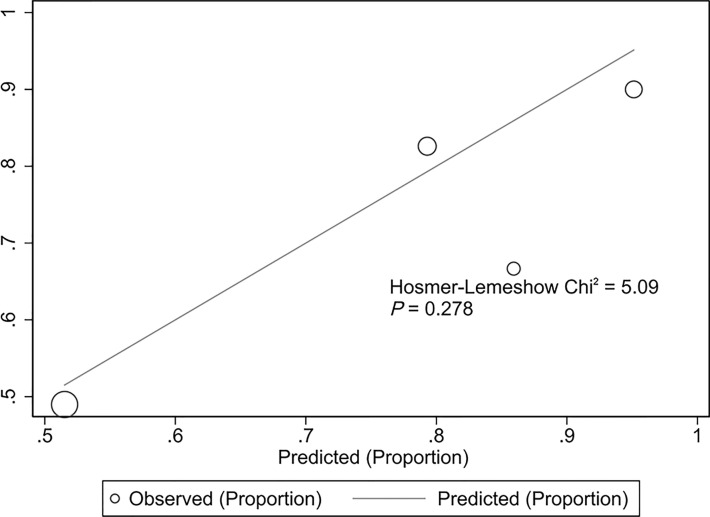
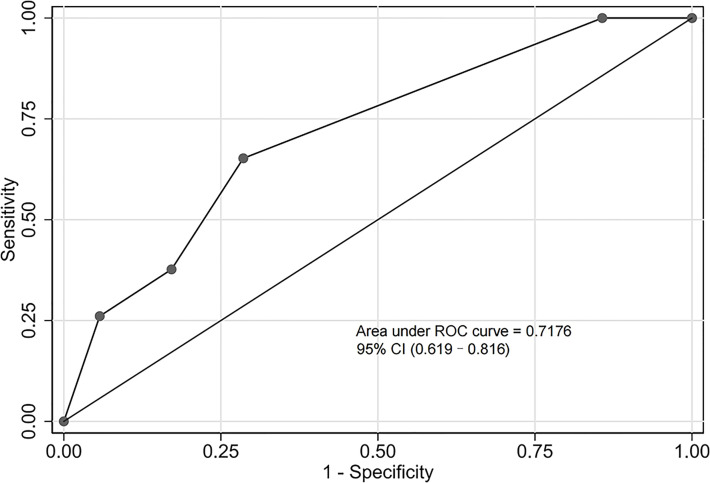
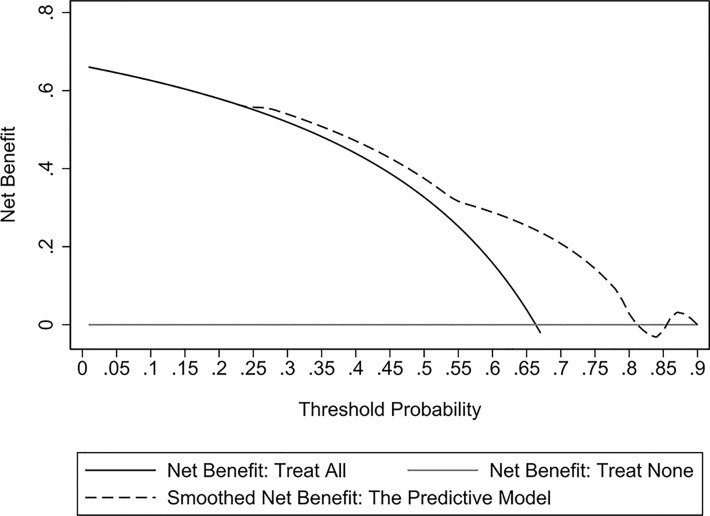
In this study, we analyzed the antibiotic resistance of carbapenem-resistant gram-negative bacteria (CR-GNB) in intensive care unit (ICU) patients and developed a predictive model. We retrospectively collected the data of patients with GNB infection admitted to the ICU of the First Affiliated Hospital of Fujian Medical University, who were then divided into a CR and a carbapenem-susceptible (CS) group for CR-GNB infection analysis. Patients admitted between December 1, 2017, and July 31, 2019, were assigned to the experimental cohort (n = 205), and their data were subjected to multivariate logistic regression analysis to identify independent risk factors for constructing the nomogram-based predictive model. Patients admitted between August 1, 2019, and September 1, 2020, were assigned to the validation cohort for validating the predictive model (n = 104). The Hosmer-Lemeshow test and receiver operating characteristic (ROC) curve analysis were used to validate the model's performance. Overall, 309 patients with GNB infection were recruited. Of them, 97 and 212 were infected with CS-GNB and CR-GNB, respectively. Carbapenem-resistant Klebsiella pneumoniae (CRKP), carbapenem-resistant Acinetobacter baumannii (CRAB) and carbapenem-resistant Pseudomonas aeruginosa (CRPA) were the most prevalent CR-GNB. The multivariate logistic regression analysis results of the experimental cohort revealed that a history of combination antibiotic treatments (OR: 3.197, 95% CI: 1.561-6.549), hospital-acquired infection (OR: 3.563, 95% CI: 1.062-11.959) and mechanical ventilation ≥ 7 days (OR: 5.096, 95% CI: 1.865-13.923) were independent risk factors for CR-GNB infection, which were then used for nomogram construction. The model demonstrated a good fit of observed data (p = 0.999), with an area under the ROC curve (AUC) of 0.753 (95% CI: 0.685-0.820) and 0.718 (95% CI: 0.619-0.816) for the experimental and validation cohort, respectively. The decision curve analysis results suggested that the model has a high practical value for clinical practice. The Hosmer-Lemeshow test indicated a good fit of the model in the validation cohort (p-value, 0.278). Overall, our proposed predictive model exhibited a good predictive value in identifying patients at high risk of developing CR-GNB infection in the ICU and could be used to guide preventive and treatment measures.
Keywords: area under the receiver operating characteristic curve; carbapenem-resistant gram-negative bacteria; logistic regression; predictive model; risk factor.
Copyright © 2023 Liao, Feng, Lin, Zhou, Lin, Zhuo and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Aleidan F. A. S., Alkhelaifi H., Alsenaid A., Alromaizan H., Alsalham F., Almutairi A., et al. . (2021). Incidence and risk factors of carbapenem-resistant enterobacteriaceae infection in intensive care units: A matched case-control study. Expert Rev. Anti Infect. Ther. 19, 393–398. doi: 10.1080/14787210.2020.1822736 - DOI - PubMed
-
- CLSI (2017). Performance standards for antimicrobial susceptibility testing (Wayne PA: Clinical and Laboratory Standards Institute; ), M100–MS27.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical