

Integrated genetic and clinical prognostic factors for aggressive adult T-cell leukemia/lymphoma
- PMID: 36794502
- PMCID: PMC10388278
- DOI: 10.3324/haematol.2022.281510
Integrated genetic and clinical prognostic factors for aggressive adult T-cell leukemia/lymphoma
Abstract
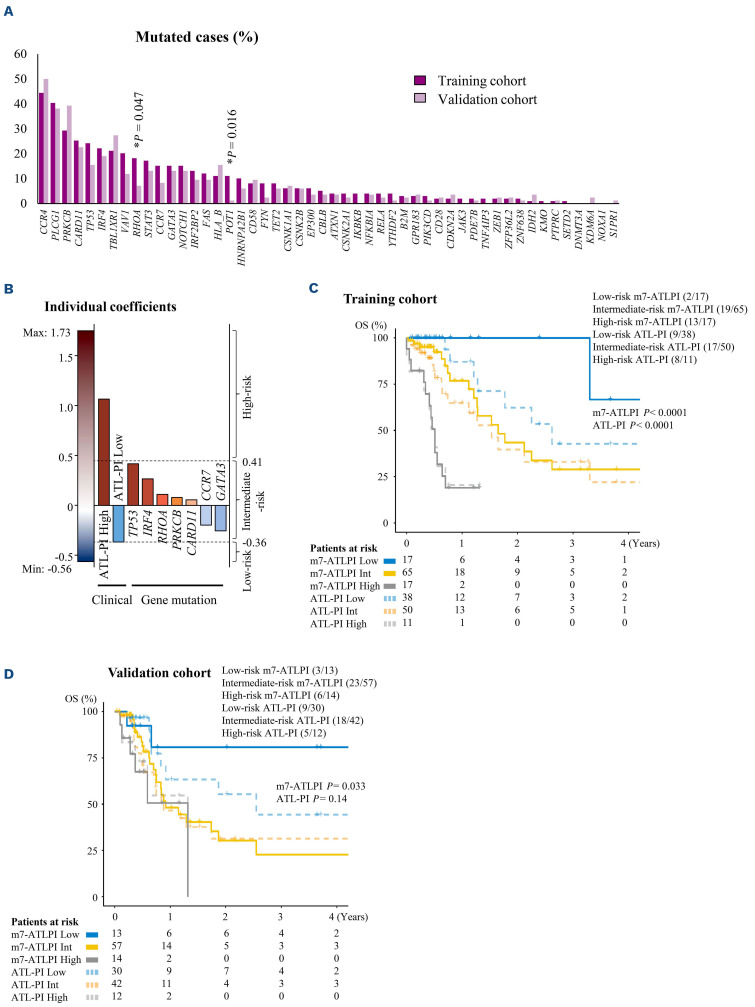
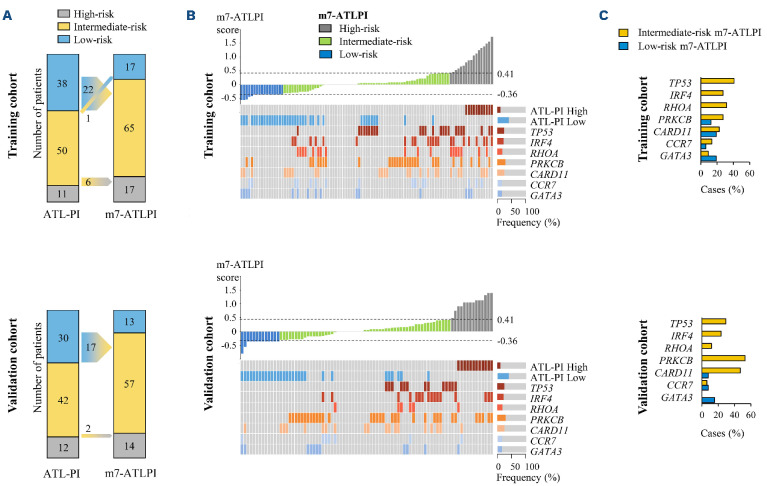
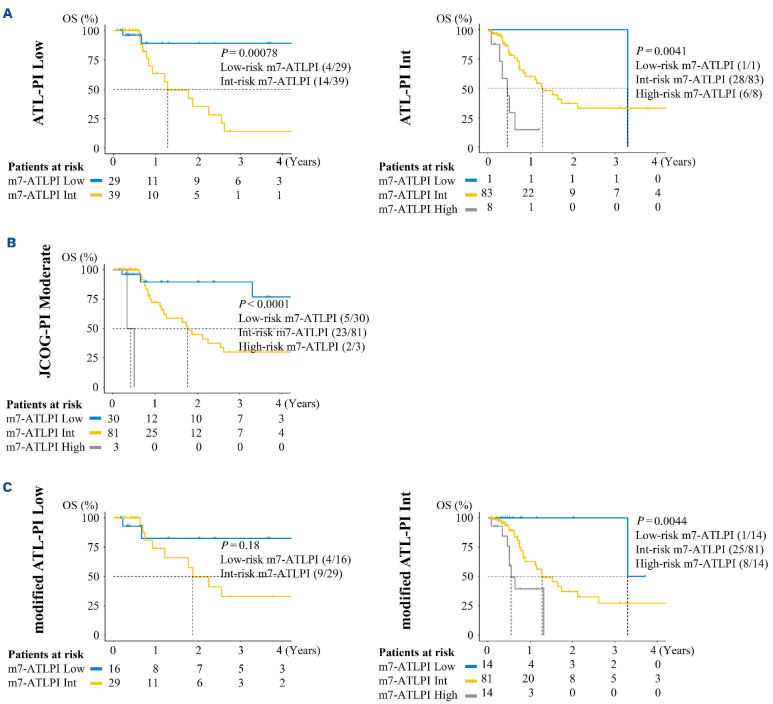
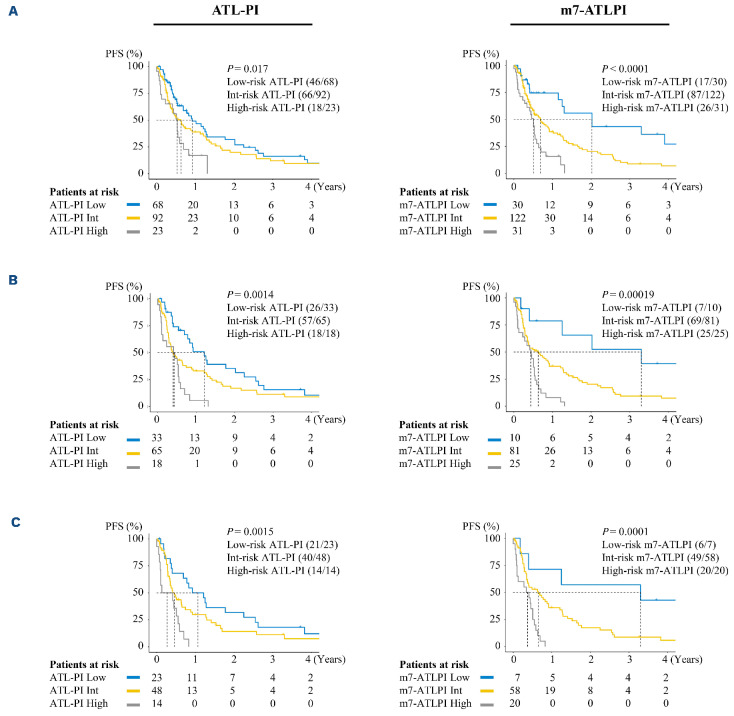
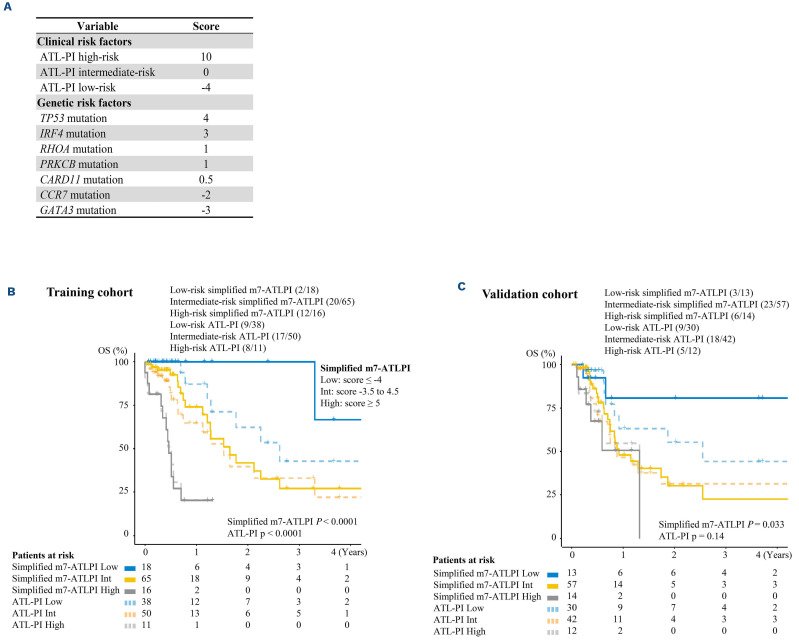
The prognosis of aggressive adult T-cell leukemia/lymphoma (ATL) is poor, and allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a curative treatment. In order to identify favorable prognostic patients after intensive chemotherapy, and who therefore might not require upfront allo-HSCT, we aimed to improve risk stratification of aggressive ATL patients aged <70 years. The clinical risk factors and genetic mutations were incorporated into risk modeling for overall survival (OS). We generated the m7-ATLPI, a clinicogenetic risk model for OS, that included the ATL prognostic index (PI) (ATL-PI) risk category, and non-silent mutations in seven genes, namely TP53, IRF4, RHOA, PRKCB, CARD11, CCR7, and GATA3. In the training cohort of 99 patients, the m7-ATLPI identified a low-, intermediate-, and highrisk group with 2-year OS of 100%, 43%, and 19%, respectively (hazard ratio [HR] =5.46; P<0.0001). The m7-ATLPI achieved superior risk stratification compared to the current ATL-PI (C-index 0.92 vs. 0.85, respectively). In the validation cohort of 84 patients, the m7-ATLPI defined low-, intermediate-, and high-risk groups with a 2-year OS of 81%, 30%, and 0%, respectively (HR=2.33; P=0.0094), and the model again outperformed the ATL-PI (C-index 0.72 vs. 0.70, respectively). The simplified m7-ATLPI, which is easier to use in clinical practice, achieved superior risk stratification compared to the ATLPI, as did the original m7-ATLPI; the simplified version was calculated by summing the following: high-risk ATL-PI category (+10), low-risk ATL-PI category (-4), and non-silent mutations in TP53 (+4), IRF4 (+3), RHOA (+1), PRKCB (+1), CARD11 (+0.5), CCR7 (-2), and GATA3 (-3).
Figures
References
-
- Uchiyama T, Yodoi J, Sagawa K, et al. . Adult T-cell leukemia: clinical and hematologic features of 16 cases. Blood. 1977;50(3):481-492. - PubMed
-
- Shimoyama M. Diagnostic criteria and classification of clinical subtypes of adult T-cell leukaemia-lymphoma. A report from the Lymphoma Study Group (1984-87). Br J Haematol. 1991;79(3):428-437. - PubMed
-
- Shimoyama M. Chemotherapy of ATL. K Takatsuki (Ed), Adult T-Cell Leukemia, Oxford University Press. Oxford. 1994:221-227.
-
- Tsukasaki K, Utsunomiya A, Fukuda H, et al. . VCAP-AMP-VECP compared with biweekly CHOP for adult T-cell leukemia-lymphoma: Japan Clinical Oncology Group Study JCOG9801. J Clin Oncol. 2007;25(34):5458-5464. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
