

Neurological complications of sepsis
- PMID: 36794932
- PMCID: PMC9994816
- DOI: 10.1097/MCC.0000000000001022
Neurological complications of sepsis
Abstract
Purpose of review: Sepsis, defined as life-threatening organ dysfunction caused by a dysregulated host response to infection, is a leading cause of hospital and ICU admission. The central and peripheral nervous system may be the first organ system to show signs of dysfunction, leading to clinical manifestations such as sepsis-associated encephalopathy (SAE) with delirium or coma and ICU-acquired weakness (ICUAW). In the current review, we want to highlight developing insights into the epidemiology, diagnosis, prognosis, and treatment of patients with SAE and ICUAW.
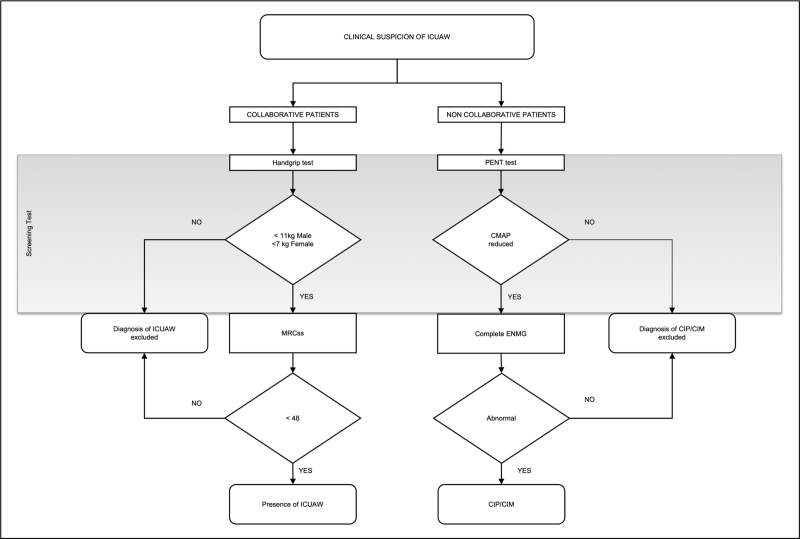
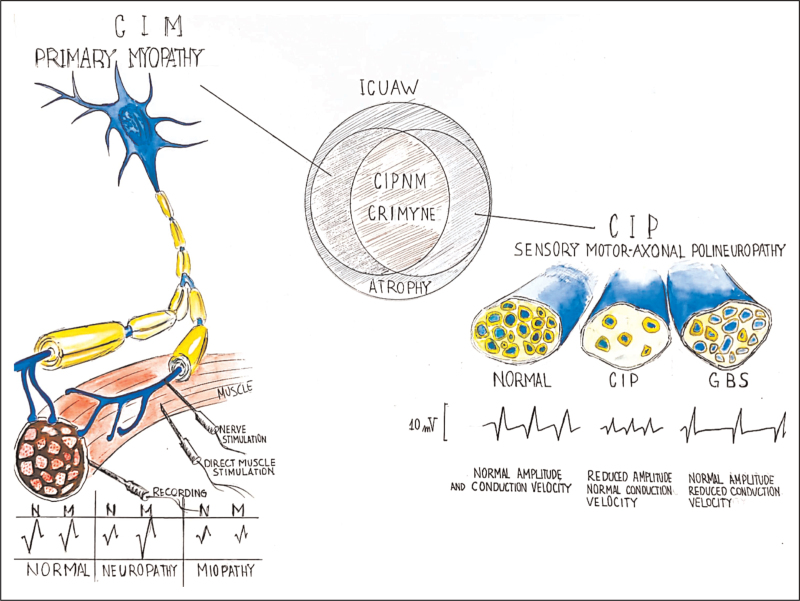
Recent findings: The diagnosis of neurological complications of sepsis remains clinical, although the use of electroencephalography and electromyography can support the diagnosis, especially in noncollaborative patients, and can help in defining disease severity. Moreover, recent studies suggest new insights into the long-term effects associated with SAE and ICUAW, highlighting the need for effective prevention and treatment.
Summary: In this manuscript, we provide an overview of recent insights and developments in the prevention, diagnosis, and treatment of patients with SAE and ICUAW.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. . Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001; 29:1303–1310. - PubMed
-
- Sonneville R, de Montmollin E, Poujade J, et al. . Potentially modifiable factors contributing to sepsis-associated encephalopathy. Intensive Care Med 2017; 43:1075–1084. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
