

Deep Learning With Chest Radiographs for Making Prognoses in Patients With COVID-19: Retrospective Cohort Study
- PMID: 36795468
- PMCID: PMC9937110
- DOI: 10.2196/42717
Deep Learning With Chest Radiographs for Making Prognoses in Patients With COVID-19: Retrospective Cohort Study
Erratum in
-
Correction: Deep Learning With Chest Radiographs for Making Prognoses in Patients With COVID-19: Retrospective Cohort Study.J Med Internet Res. 2023 Aug 23;25:e51951. doi: 10.2196/51951. J Med Internet Res. 2023. PMID: 37611252 Free PMC article.
Abstract
Background: An artificial intelligence (AI) model using chest radiography (CXR) may provide good performance in making prognoses for COVID-19.
Objective: We aimed to develop and validate a prediction model using CXR based on an AI model and clinical variables to predict clinical outcomes in patients with COVID-19.
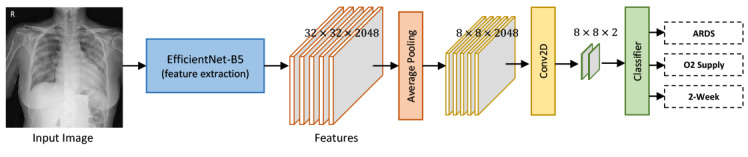
Methods: This retrospective longitudinal study included patients hospitalized for COVID-19 at multiple COVID-19 medical centers between February 2020 and October 2020. Patients at Boramae Medical Center were randomly classified into training, validation, and internal testing sets (at a ratio of 8:1:1, respectively). An AI model using initial CXR images as input, a logistic regression model using clinical information, and a combined model using the output of the AI model (as CXR score) and clinical information were developed and trained to predict hospital length of stay (LOS) ≤2 weeks, need for oxygen supplementation, and acute respiratory distress syndrome (ARDS). The models were externally validated in the Korean Imaging Cohort of COVID-19 data set for discrimination and calibration.
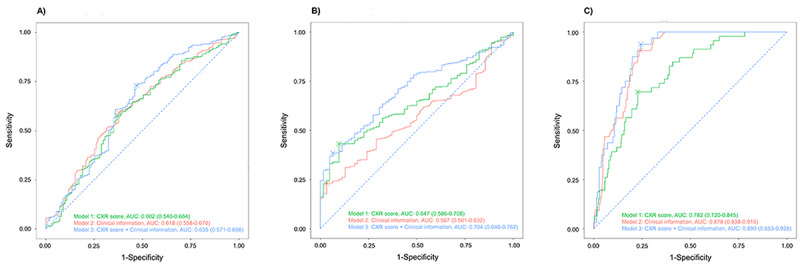
Results: The AI model using CXR and the logistic regression model using clinical variables were suboptimal to predict hospital LOS ≤2 weeks or the need for oxygen supplementation but performed acceptably in the prediction of ARDS (AI model area under the curve [AUC] 0.782, 95% CI 0.720-0.845; logistic regression model AUC 0.878, 95% CI 0.838-0.919). The combined model performed better in predicting the need for oxygen supplementation (AUC 0.704, 95% CI 0.646-0.762) and ARDS (AUC 0.890, 95% CI 0.853-0.928) compared to the CXR score alone. Both the AI and combined models showed good calibration for predicting ARDS (P=.079 and P=.859).
Conclusions: The combined prediction model, comprising the CXR score and clinical information, was externally validated as having acceptable performance in predicting severe illness and excellent performance in predicting ARDS in patients with COVID-19.
Keywords: AI model; COVID-19; artificial intelligence; clinical outcome; deep learning; machine learning; medical imaging; prediction model; prognosis; radiography, thoracic.
©Hyun Woo Lee, Hyun Jun Yang, Hyungjin Kim, Ue-Hwan Kim, Dong Hyun Kim, Soon Ho Yoon, Soo-Youn Ham, Bo Da Nam, Kum Ju Chae, Dabee Lee, Jin Young Yoo, So Hyeon Bak, Jin Young Kim, Jin Hwan Kim, Ki Beom Kim, Jung Im Jung, Jae-Kwang Lim, Jong Eun Lee, Myung Jin Chung, Young Kyung Lee, Young Seon Kim, Sang Min Lee, Woocheol Kwon, Chang Min Park, Yun-Hyeon Kim, Yeon Joo Jeong, Kwang Nam Jin, Jin Mo Goo. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 16.02.2023.
Conflict of interest statement
Conflicts of Interest: HK received consulting fees from Radisen; holds stock and stock options in MEDICALIP. Outside this study, SHY works as a chief medical officer in the MEDICAL IP.
Figures
Similar articles
-
Initial chest radiographs and artificial intelligence (AI) predict clinical outcomes in COVID-19 patients: analysis of 697 Italian patients.Eur Radiol. 2021 Mar;31(3):1770-1779. doi: 10.1007/s00330-020-07269-8. Epub 2020 Sep 18. Eur Radiol. 2021. PMID: 32945968 Free PMC article.
-
Multi-center validation of an artificial intelligence system for detection of COVID-19 on chest radiographs in symptomatic patients.Eur Radiol. 2023 Jan;33(1):23-33. doi: 10.1007/s00330-022-08969-z. Epub 2022 Jul 2. Eur Radiol. 2023. PMID: 35779089
-
Prognostication of patients with COVID-19 using artificial intelligence based on chest x-rays and clinical data: a retrospective study.Lancet Digit Health. 2021 May;3(5):e286-e294. doi: 10.1016/S2589-7500(21)00039-X. Epub 2021 Mar 24. Lancet Digit Health. 2021. PMID: 33773969 Free PMC article.
-
A narrative review on characterization of acute respiratory distress syndrome in COVID-19-infected lungs using artificial intelligence.Comput Biol Med. 2021 Mar;130:104210. doi: 10.1016/j.compbiomed.2021.104210. Epub 2021 Jan 18. Comput Biol Med. 2021. PMID: 33550068 Free PMC article. Review.
-
Machine and Deep Learning for Tuberculosis Detection on Chest X-Rays: Systematic Literature Review.J Med Internet Res. 2023 Jul 3;25:e43154. doi: 10.2196/43154. J Med Internet Res. 2023. PMID: 37399055 Free PMC article.
Cited by
-
The role of artificial intelligence in pandemic responses: from epidemiological modeling to vaccine development.Mol Biomed. 2025 Jan 3;6(1):1. doi: 10.1186/s43556-024-00238-3. Mol Biomed. 2025. PMID: 39747786 Free PMC article. Review.
-
Accuracy of artificial intelligence algorithms in predicting acute respiratory distress syndrome: a systematic review and meta-analysis.BMC Med Inform Decis Mak. 2025 Jan 28;25(1):44. doi: 10.1186/s12911-025-02869-0. BMC Med Inform Decis Mak. 2025. PMID: 39875868 Free PMC article.
-
The Application of Mask Region-Based Convolutional Neural Networks in the Detection of Nasal Septal Deviation Using Cone Beam Computed Tomography Images: Proof-of-Concept Study.JMIR Form Res. 2024 Sep 3;8:e57335. doi: 10.2196/57335. JMIR Form Res. 2024. PMID: 39226096 Free PMC article.
-
Unraveling complex relationships between COVID-19 risk factors using machine learning based models for predicting mortality of hospitalized patients and identification of high-risk group: a large retrospective study.Front Med (Lausanne). 2023 May 4;10:1170331. doi: 10.3389/fmed.2023.1170331. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37215714 Free PMC article.
-
A deep learning model for predicting COVID-19 ARDS in critically ill patients.Front Med (Lausanne). 2023 Jul 25;10:1221711. doi: 10.3389/fmed.2023.1221711. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37564041 Free PMC article.
References
-
- WHO coronavirus disease (COVID-19) dashboard. World Health Organization. [2023-01-30]. https://covid19.who.int .
-
- Chua F, Vancheeswaran R, Draper A, Vaghela T, Knight M, Mogal R, Singh J, Spencer LG, Thwaite E, Mitchell H, Calmonson S, Mahdi N, Assadullah S, Leung M, O'Neill A, Popat C, Kumar R, Humphries T, Talbutt R, Raghunath S, Molyneaux PL, Schechter M, Lowe J, Barlow A. Early prognostication of COVID-19 to guide hospitalisation versus outpatient monitoring using a point-of-test risk prediction score. Thorax. 2021 Jul;76(7):696–703. doi: 10.1136/thoraxjnl-2020-216425. https://europepmc.org/abstract/MED/33692174 thoraxjnl-2020-216425 - DOI - PubMed
-
- Wynants L, Van Calster B, Collins GS, Riley RD, Heinze G, Schuit E, Bonten MMJ, Dahly Darren L, Damen Johanna A A, Debray Thomas P A, de Jong Valentijn M T, De Vos Maarten, Dhiman Paul, Haller Maria C, Harhay Michael O, Henckaerts Liesbet, Heus Pauline, Kammer Michael, Kreuzberger Nina, Lohmann Anna, Luijken Kim, Ma Jie, Martin Glen P, McLernon David J, Andaur Navarro Constanza L, Reitsma Johannes B, Sergeant Jamie C, Shi Chunhu, Skoetz Nicole, Smits Luc J M, Snell Kym I E, Sperrin Matthew, Spijker René, Steyerberg Ewout W, Takada Toshihiko, Tzoulaki Ioanna, van Kuijk Sander M J, van Bussel Bas, van der Horst Iwan C C, van Royen Florien S, Verbakel Jan Y, Wallisch Christine, Wilkinson Jack, Wolff Robert, Hooft Lotty, Moons Karel G M, van Smeden Maarten. Prediction models for diagnosis and prognosis of covid-19: systematic review and critical appraisal. BMJ. 2020 Apr 07;369:m1328. doi: 10.1136/bmj.m1328. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=32265220 - DOI - PMC - PubMed
-
- Recommendations for the use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. American College of Radiology. [2023-01-30]. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recom... .
-
- Wang L, Zhang Y, Wang D, Tong X, Liu T, Zhang S, Huang J, Zhang L, Chen L, Fan H, Clarke M. Artificial intelligence for COVID-19: a systematic review. Front Med (Lausanne) 2021;8:704256. doi: 10.3389/fmed.2021.704256. https://europepmc.org/abstract/MED/34660623 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
