

Are There Differences in Postoperative Opioid Prescribing Across Racial and Ethnic Groups? Assessment of an Academic Health System
- PMID: 36795497
- PMCID: PMC10344544
- DOI: 10.1097/CORR.0000000000002596
Are There Differences in Postoperative Opioid Prescribing Across Racial and Ethnic Groups? Assessment of an Academic Health System
Abstract
Background: Previous studies have demonstrated racial disparities in opioid prescribing in emergency departments and after surgical procedures. Orthopaedic surgeons account for a large proportion of dispensed opioid prescriptions, yet there are few data investigating whether racial or ethnic disparities exist in opioid dispensing after orthopaedic procedures.
Questions/purposes: (1) Are Black, Hispanic or Latino, or Asian or Pacific Islander (PI) patients less likely than non-Hispanic White patients to receive an opioid prescription after an orthopaedic procedure in an academic United States health system? (2) Of the patients who do receive a postoperative opioid prescription, do Black, Hispanic or Latino, or Asian or PI patients receive a lower analgesic dose than non-Hispanic White patients when analyzed by type of procedure performed?
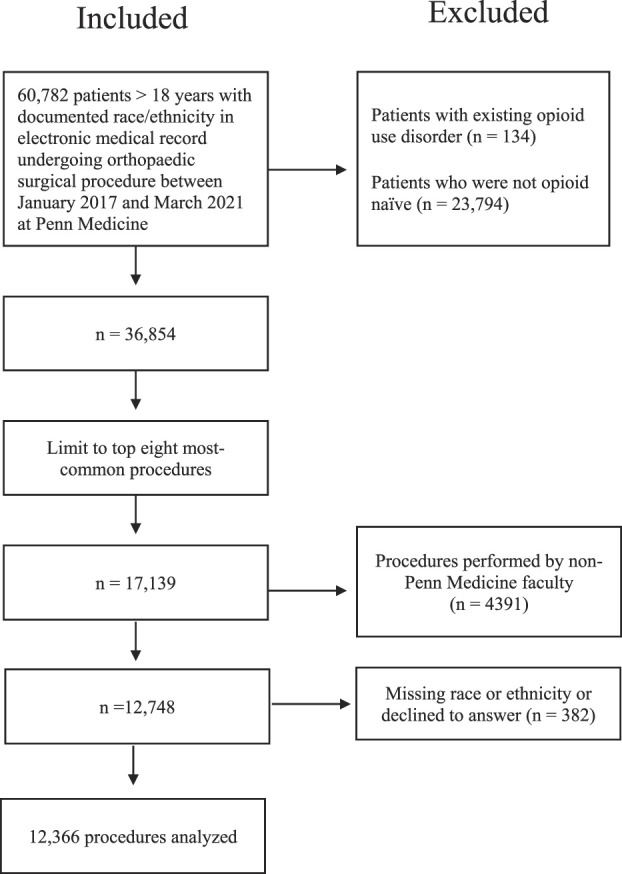
Methods: Between January 2017 and March 2021, 60,782 patients underwent an orthopaedic surgical procedure at one of the six Penn Medicine healthcare system hospitals. Of these patients, we considered patients who had not been prescribed an opioid within 1 year eligible for the study, resulting in 61% (36,854) of patients. A total of 40% (24,106) of patients were excluded because they did not undergo one of the top eight most-common orthopaedic procedures studied or their procedure was not performed by a Penn Medicine faculty member. Missing data consisted of 382 patients who had no race or ethnicity listed in their record or declined to provide a race or ethnicity; these patients were excluded. This left 12,366 patients for analysis. Sixty-five percent (8076) of patients identified as non-Hispanic White, 27% (3289) identified as Black, 3% (372) identified as Hispanic or Latino, 3% (318) identified as Asian or PI, and 3% (311) identified as another race ("other"). Prescription dosages were converted to total morphine milligram equivalents for analysis. Statistical differences in receipt of a postoperative opioid prescription were assessed with multivariate logistic regression models within procedure, adjusted for age, gender, and type of healthcare insurance. Kruskal-Wallis tests were used to assess for differences in the total morphine milligram equivalent dosage of the prescription, stratified by procedure.
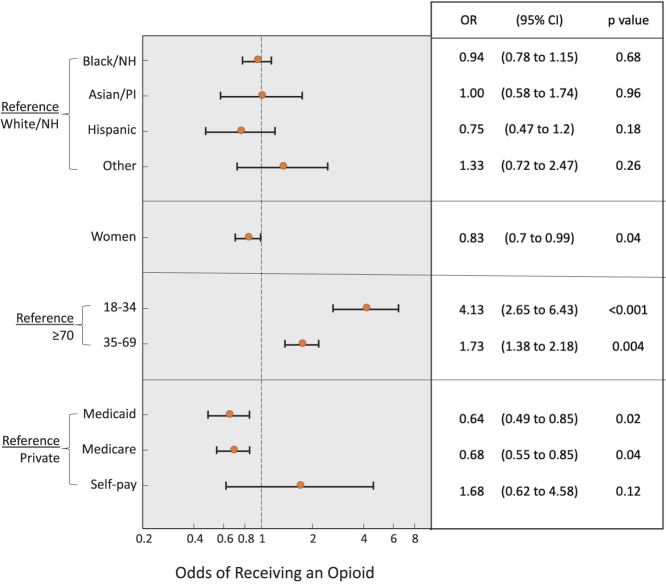
Results: Almost all patients (95% [11,770 of 12,366]) received an opioid prescription. After risk adjustment, we found no differences in the odds of Black (odds ratio 0.94 [95% confidence interval 0.78 to 1.15]; p = 0.68), Hispanic or Latino (OR 0.75 [95% CI 0.47 to 1.20]; p = 0.18), Asian or PI (OR 1.00 [95% CI 0.58 to 1.74]; p = 0.96), or other-race patients (OR 1.33 [95% CI 0.72 to 2.47]; p = 0.26) receiving a postoperative opioid prescription compared with non-Hispanic White patients. There were no race or ethnicity differences in the median morphine milligram equivalent dose of postoperative opioid analgesics prescribed (p > 0.1 for all eight procedures) based on procedure.
Conclusion: In this academic health system, we did not find any differences in opioid prescribing after common orthopaedic procedures by patient race or ethnicity. A potential explanation is the use of surgical pathways in our orthopaedic department. Formal standardized opioid prescribing guidelines may reduce variability in opioid prescribing.
Level of evidence: Level III, therapeutic study.
Copyright © 2023 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Are There Differences in Postoperative Opioid Prescribing Across Racial and Ethnic Groups? Assessment of an Academic Health System.Clin Orthop Relat Res. 2023 Aug 1;481(8):1512-1514. doi: 10.1097/CORR.0000000000002655. Epub 2023 Apr 7. Clin Orthop Relat Res. 2023. PMID: 37026860 Free PMC article. No abstract available.
Similar articles
-
Racial and Ethnic Disparities in Opioid Prescribing on Hospital Discharge Among Older Adults: A National Retrospective Cohort Study.J Gen Intern Med. 2024 Jun;39(8):1444-1451. doi: 10.1007/s11606-024-08687-w. Epub 2024 Feb 29. J Gen Intern Med. 2024. PMID: 38424348 Free PMC article.
-
Association of Race and Ethnicity With Postoperative Gabapentinoid and Opioid Prescribing Trends for Older Adults.J Surg Res. 2024 Jun;298:47-52. doi: 10.1016/j.jss.2024.02.017. Epub 2024 Mar 29. J Surg Res. 2024. PMID: 38554545 Free PMC article.
-
Racial inequities in U.S. naloxone prescriptions.Subst Abus. 2020;41(2):232-244. doi: 10.1080/08897077.2019.1686721. Epub 2019 Nov 13. Subst Abus. 2020. PMID: 31718487
-
Postoperative Opioid Prescription Practices at Discharge for Pediatric Orthopaedic Patients: A Systematic Review.J Pediatr Soc North Am. 2024 Sep 24;9:100123. doi: 10.1016/j.jposna.2024.100123. eCollection 2024 Nov. J Pediatr Soc North Am. 2024. PMID: 40432670 Free PMC article. Review.
-
Racial and ethnic disparity in shoulder surgery: a systematic review.J Shoulder Elbow Surg. 2025 Jan;34(1):203-211. doi: 10.1016/j.jse.2024.06.013. Epub 2024 Aug 3. J Shoulder Elbow Surg. 2025. PMID: 39103086
Cited by
-
Disparities in Postoperative Pain Management: A Scoping Review of Prescription Practices and Social Determinants of Health.Pharmacy (Basel). 2025 Feb 24;13(2):34. doi: 10.3390/pharmacy13020034. Pharmacy (Basel). 2025. PMID: 40126307 Free PMC article. Review.
References
-
- Artiga S, Hill L, Damico A. Health coverage by race and ethnicity, 2010-2021. Available at: https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-c.... Accessed October 2, 2022.
-
- Glance LG, Wissler R., Glantz C, Osler TM, Mukamel DB, Dick AW. Racial differences in the use of epidural analgesia for labor. Anesthesiology. 2007;106:19-25. - PubMed
-
- Herb JN, Williams BM, Chen KA, et al. The impact of standard postoperative opioid prescribing guidelines on racial differences in opioid prescribing: a retrospective review. Surgery. 2021;170:180-185. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
