

The Evolving Pediatric HIV Epidemic in Rural Southern Zambia: The Beneficial Impact of Advances in Prevention and Treatment at a District Hospital From 2007 to 2019
- PMID: 36795584
- PMCID: PMC10360039
- DOI: 10.1097/INF.0000000000003873
The Evolving Pediatric HIV Epidemic in Rural Southern Zambia: The Beneficial Impact of Advances in Prevention and Treatment at a District Hospital From 2007 to 2019
Abstract
Background: Remarkable progress has been made in expanding access to services addressing the pediatric HIV epidemic, including programs to prevent mother-to-child transmission, early diagnosis and treatment for children living with HIV. Few long-term data are available from rural sub-Saharan Africa to assess implementation and impact of national guidelines.
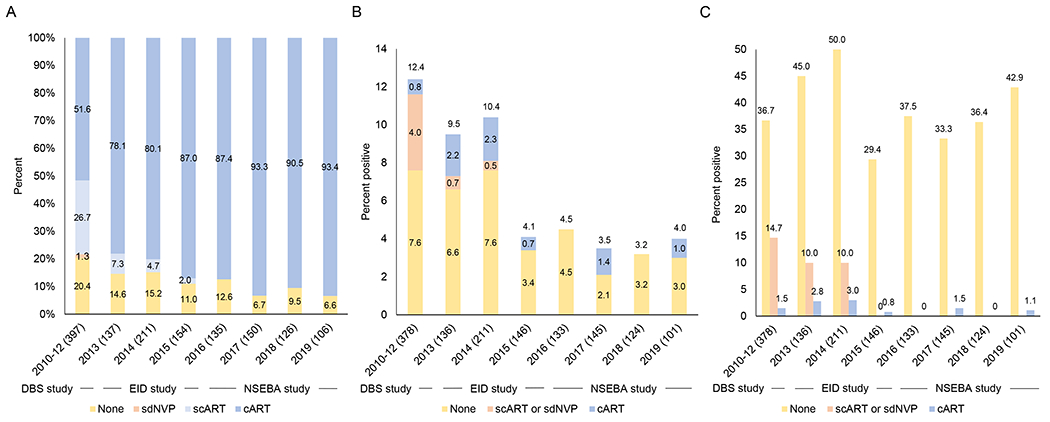
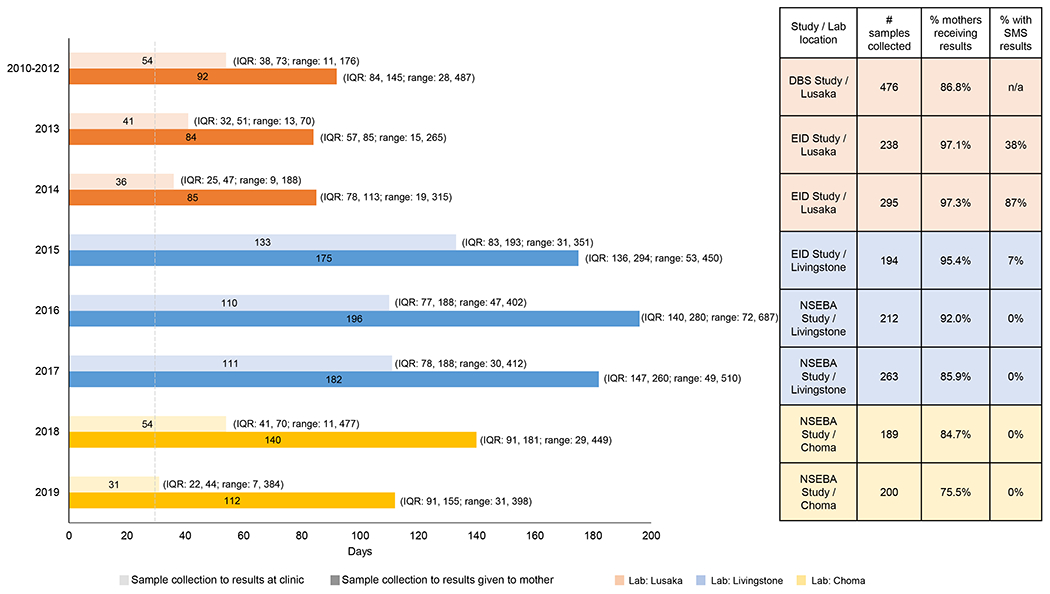
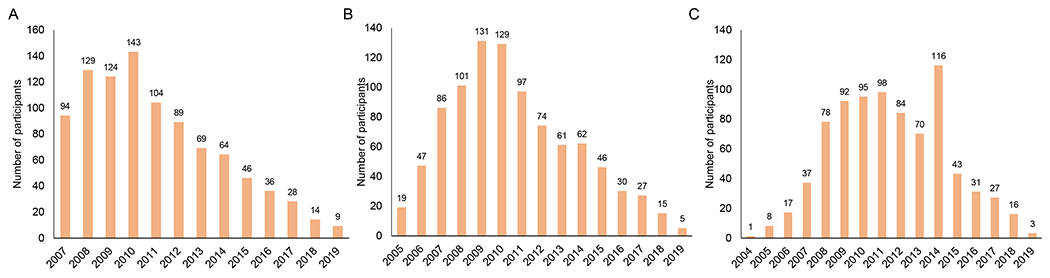
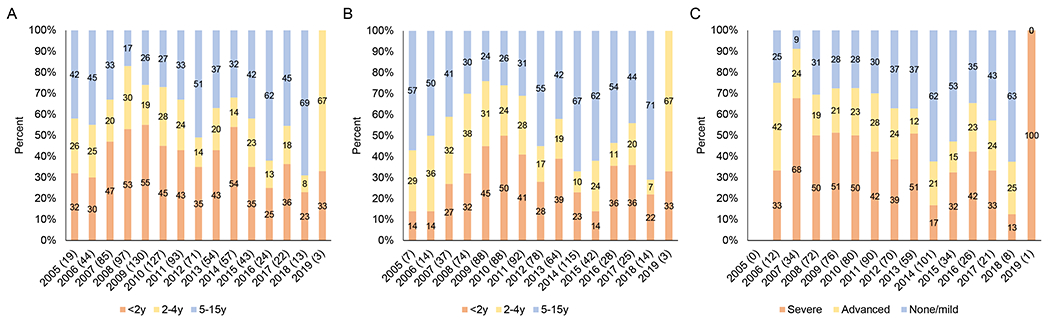
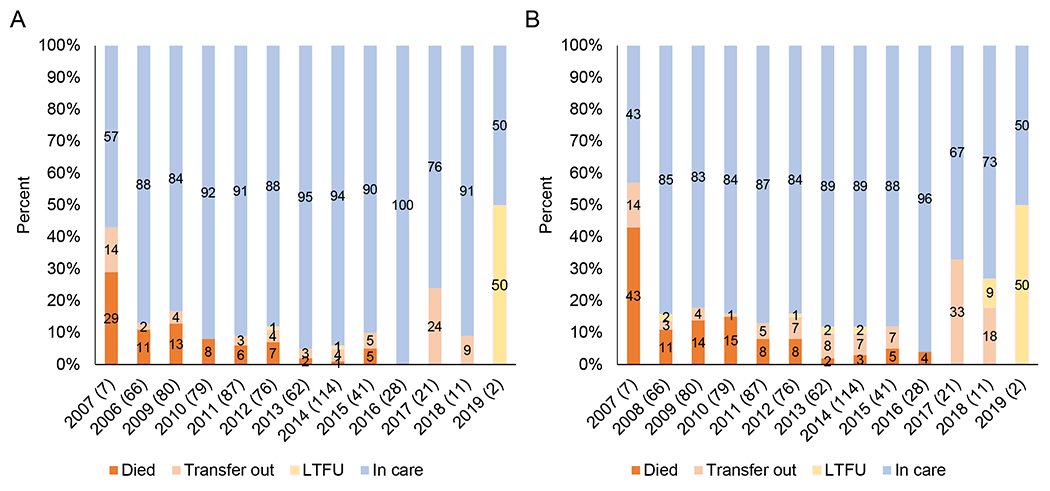
Methods: Results from 3 cross-sectional studies and 1 cohort study conducted at Macha Hospital in Southern Province, Zambia from 2007 to 2019 were summarized. For infant diagnosis, maternal antiretroviral treatment, infant test results and turnaround times for results were evaluated by year. For pediatric HIV care, the number and age of children initiating care and treatment, and treatment outcomes within 12 months were evaluated by year.
Results: Receipt of maternal combination antiretroviral treatment increased from 51.6% in 2010-2012 to 93.4% in 2019, and the proportion of infants testing positive decreased from 12.4% to 4.0%. Turnaround times for results returning to clinic varied but were shorter when labs consistently used a text messaging system. The proportion of mothers receiving results was higher when a text message intervention was piloted. The number of children living with HIV enrolled into care and the proportion initiating treatment with severe immunosuppression and dying within 12 months decreased over time.
Conclusions: These studies demonstrate the long-term beneficial impact of implementing a strong HIV prevention and treatment program. While expansion and decentralization brought challenges, the program succeeded in decreasing the rate of mother-to-child transmission and ensuring that children living with HIV benefit from access to life-saving treatment.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- UNAIDS. Fact Sheet - Global HIV Statistics. 2020. https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_... (accessed September 11 2020).
-
- UNAIDS. Global AIDS Update 2020: Seizing the moment. Tackling entrenched inequalities to end epidemics. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS (UNAIDS), 2021.
-
- UNAIDS. Global Plan Towards the Elimination of new HIV Infections Among Children by 2015 and Keeping Their Mothers Alive. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS, 2011.
-
- UNAIDS. UNAIDS data 2019. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS (UNAIDS), 2019.
-
- UNAIDS. Country Factsheets Zambia 2021. https://www.unaids.org/en/regionscountries/countries/zambia (accessed November 13 2022).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
