

Multicenter phase 2 study of oral azacitidine (CC-486) plus CHOP as initial treatment for PTCL
- PMID: 36796016
- PMCID: PMC10356559
- DOI: 10.1182/blood.2022018254
Multicenter phase 2 study of oral azacitidine (CC-486) plus CHOP as initial treatment for PTCL
Abstract
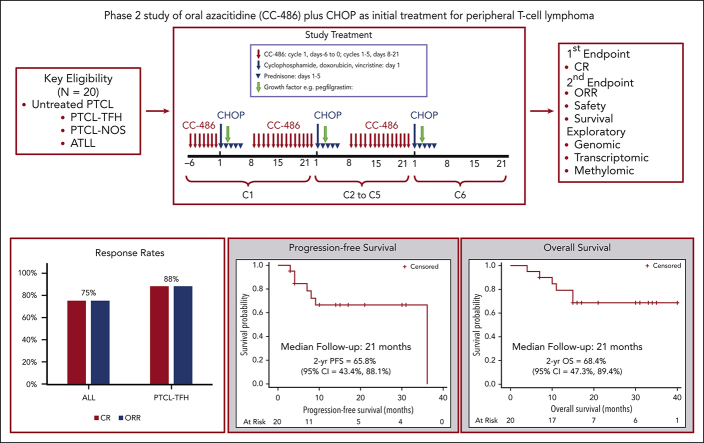
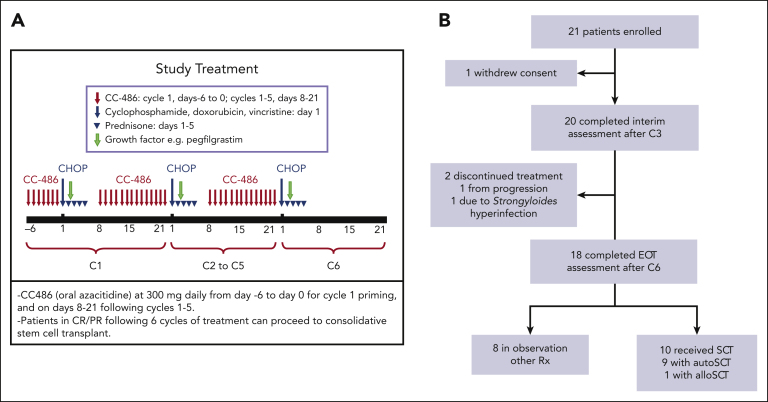
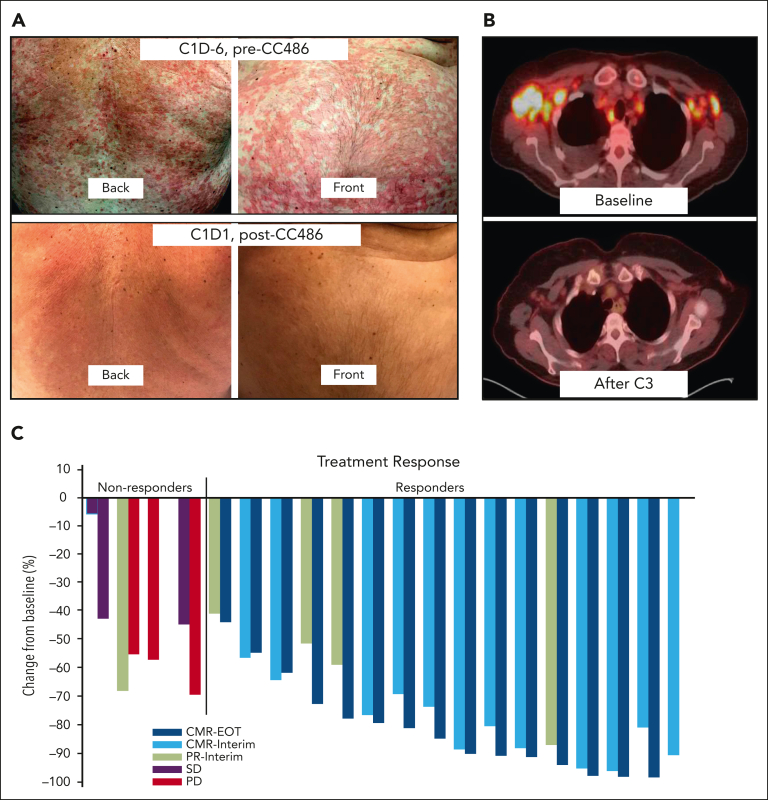
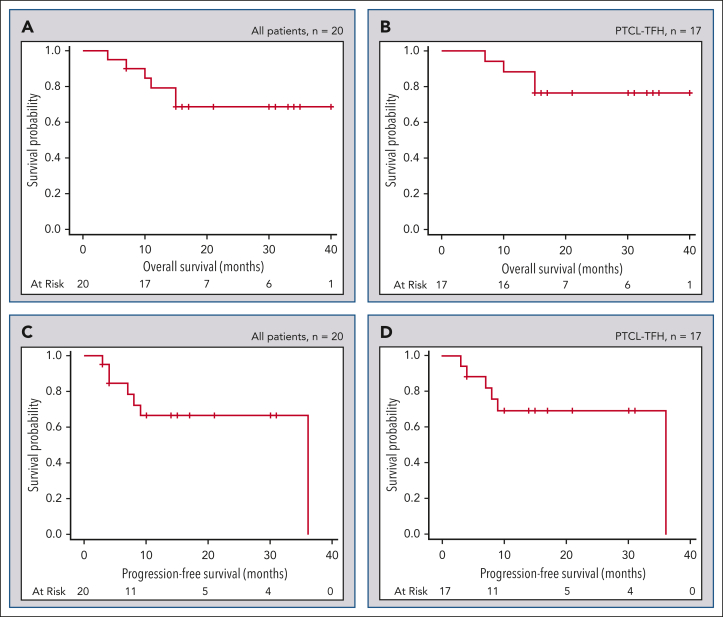
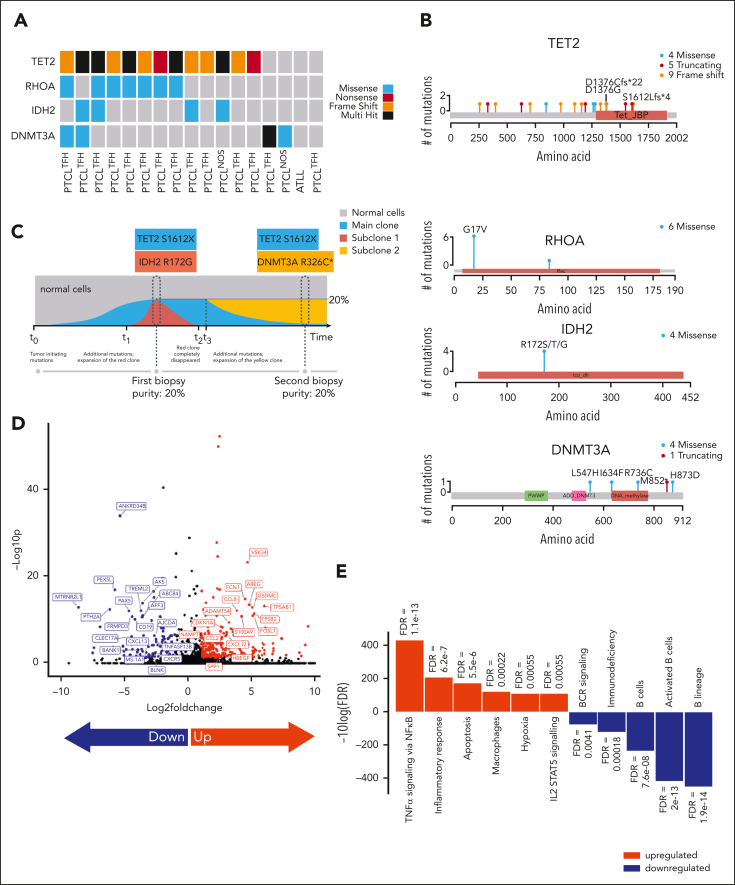
Peripheral T-cell lymphomas (PTCL) with T-follicular helper phenotype (PTCL-TFH) has recurrent mutations affecting epigenetic regulators, which may contribute to aberrant DNA methylation and chemoresistance. This phase 2 study evaluated oral azacitidine (CC-486) plus cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) as initial treatment for PTCL. CC-486 at 300 mg daily was administered for 7 days before C1 of CHOP, and for 14 days before CHOP C2-6. The primary end point was end-of-treatment complete response (CR). Secondary end points included safety and survival. Correlative studies assessed mutations, gene expression, and methylation in tumor samples. Grade 3 to 4 hematologic toxicities were mostly neutropenia (71%), with febrile neutropenia uncommon (14%). Nonhematologic toxicities included fatigue (14%) and gastrointestinal symptoms (5%). In 20 evaluable patients, CR was 75%, including 88.2% for PTCL-TFH (n = 17). The 2-year progression-free survival (PFS) was 65.8% for all and 69.2% for PTCL-TFH, whereas 2-year overall survival (OS) was 68.4% for all and 76.1% for PTCL-TFH. The frequencies of the TET2, RHOA, DNMT3A, and IDH2 mutations were 76.5%, 41.1%, 23.5%, and 23.5%, respectively, with TET2 mutations significantly associated with CR (P = .007), favorable PFS (P = .004) and OS (P = .015), and DNMT3A mutations associated with adverse PFS (P = .016). CC-486 priming contributed to the reprograming of the tumor microenvironment by upregulation of genes related to apoptosis (P < .01) and inflammation (P < .01). DNA methylation did not show significant shift. This safe and active regimen is being further evaluated in the ALLIANCE randomized study A051902 in CD30-negative PTCL. This trial was registered at www.clinicaltrials.gov as #NCT03542266.
© 2023 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: J.R. has received research support from BMS/Celgene, AstraZeneca, Genentech, Daiichi Sankyo, Pharmacyclics, and Seattle Genetics, as well as honorarium for service as a consultant for BMS/Celgene, Seattle Genetics, Secura Bio, Daiichi Sankyo, AstraZeneca, and Kite Pharma. A.M. has received research support from ADC Therapeutics, BeiGene, Miragen, Seattle Genetics, Merck, Bristol-Myers Squibb, Incyte, and SecuraBio, as well as honorarium for service as a consultant for Affimed, Imbrium Therapeutics L.P./Purdue, Janpix Ltd, Merck, Seattle Genetics, and Takeda. N.M.-S. has received research support from AstraZeneca, Bristol-Myers Squibb, Celgene, C4 Therapeutics, Corvus Pharmaceuticals, Daiichi Sankyo, Genentech/Roche, Innate Pharmaceuticals, Secura Bio/Verastem, as well as honorarium for service as a consultant for Secura Bio/Verastem, Daiichi Sankyo, C4 Therapeutics, Genentech, Karyopharm Therapeutics, Kyowa Hakko Kirin, and Ono pharmaceuticals. L.S. has received research support from Kyowa-Kirin, and EUSA Pharma, as well as honorarium for service as a consultant for Kyowa-Kirin, Daiichi Sankyo, Dren-Bio, and Secura Bio. S.H. has received research support from ADC Therapeutics, Affimed, Celgene, Crispr Therapeutics, Daiichi Sankyo, Kyowa Hakko Kirin, Millennium /Takeda, Seattle Genetics, C4, and Verastem/SecuraBio, as well as honorarium for service as a consultant for Affimed, Abcuro, Cimieo Therapeutics, Daiichi Sankyo, Kyowa Hakko Kirin, ONO Pharmaceuticals, SecuraBio, Shoreline Biosciences, Inc, Takeda, Yingli Pharma Limited, Auxilius Pharma, Myeloid Therapeutics, Acrotech, and Tubulis. S.C.R. has received research support from Genentech and Karyopharm, as well as honorarium for service as a consultant for ADC Therapeutics, Genmab, Karyopharm, Kite, and Seagen. P.M. has served as a consultant for AstraZeneca, BeiGene, BMS/Celgene, Daiichi Sankyo, Epizyme, Genentech, Janssen, Merck, and Takeda. J.P.L. has received research support from Janssen, Genentech, Epizyme, the Leukemia and Lymphoma Society, as well as honorarium for service as a consult for AbbVie, Astellas, AstraZeneca, Bayer, BeiGene, BMS, Calithera, Constellation, Eisai, Lilly, Epizyme, Genmab, Grail, Incyte, Janssen, Karyopharm, Merck, Mustang Bio, Pfizer, Roche/Genentech, Second Genome, Sutro, and Caribou Biosciences. The remaining authors declare no competing financial interests.
Figures
Comment in
-
Is it prime time for T-cell lymphoma?Blood. 2023 May 4;141(18):2161-2163. doi: 10.1182/blood.2023020004. Blood. 2023. PMID: 37140951 No abstract available.
References
-
- Vose J, Armitage J, Weisenburger D, International T-Cell Lymphoma Project International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008;26(25):4124–4130. - PubMed
-
- Reimer P, Rüdiger T, Geissinger E, et al. Autologous stem-cell transplantation as first-line therapy in peripheral T-cell lymphomas: results of a Prospective Multicenter Study. J Clin Oncol. 2009;27(1):106–113. - PubMed
-
- Simon A, Peoch M, Casassus P, et al. Upfront VIP-reinforced-ABVD (VIP-rABVD) is not superior to CHOP/21 in newly diagnosed peripheral T cell lymphoma. Results of the randomized phase III trial GOELAMS-LTP95. Br J Haematol. 2010;151(2):159–166. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
