

Proof-of-concept: SCENTinel 1.1 rapidly discriminates COVID-19-related olfactory disorders
- PMID: 36796784
- PMCID: PMC9935080
- DOI: 10.1093/chemse/bjad002
Proof-of-concept: SCENTinel 1.1 rapidly discriminates COVID-19-related olfactory disorders
Abstract
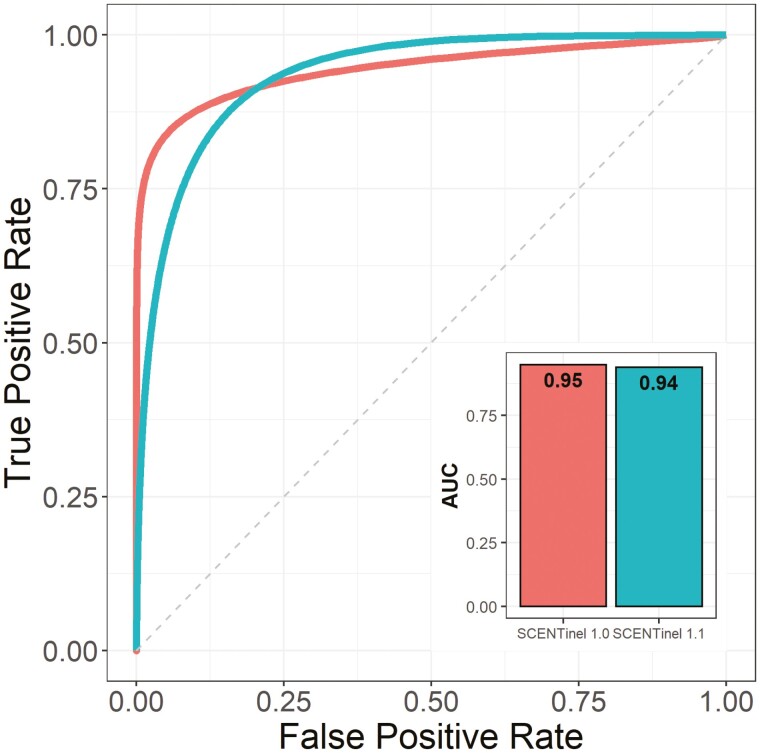
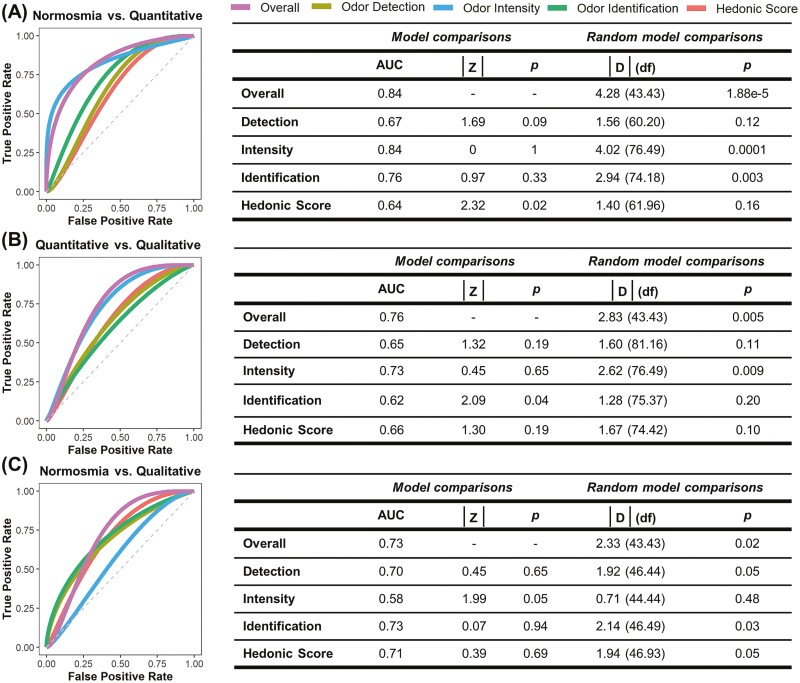
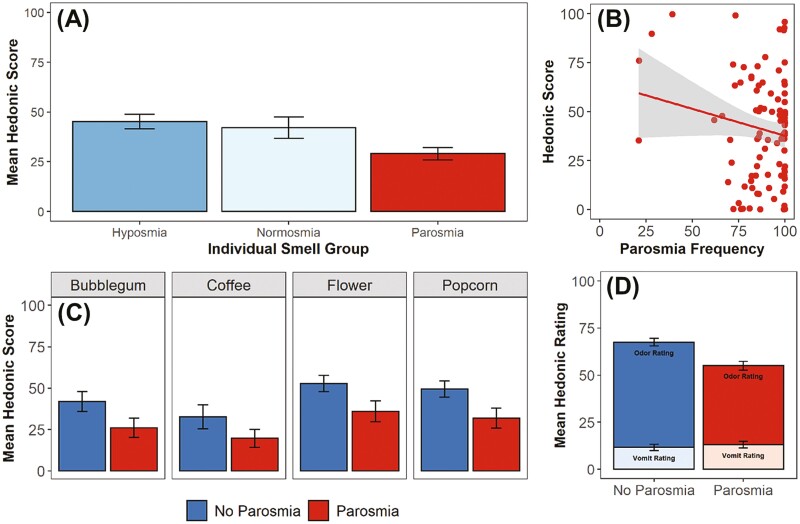
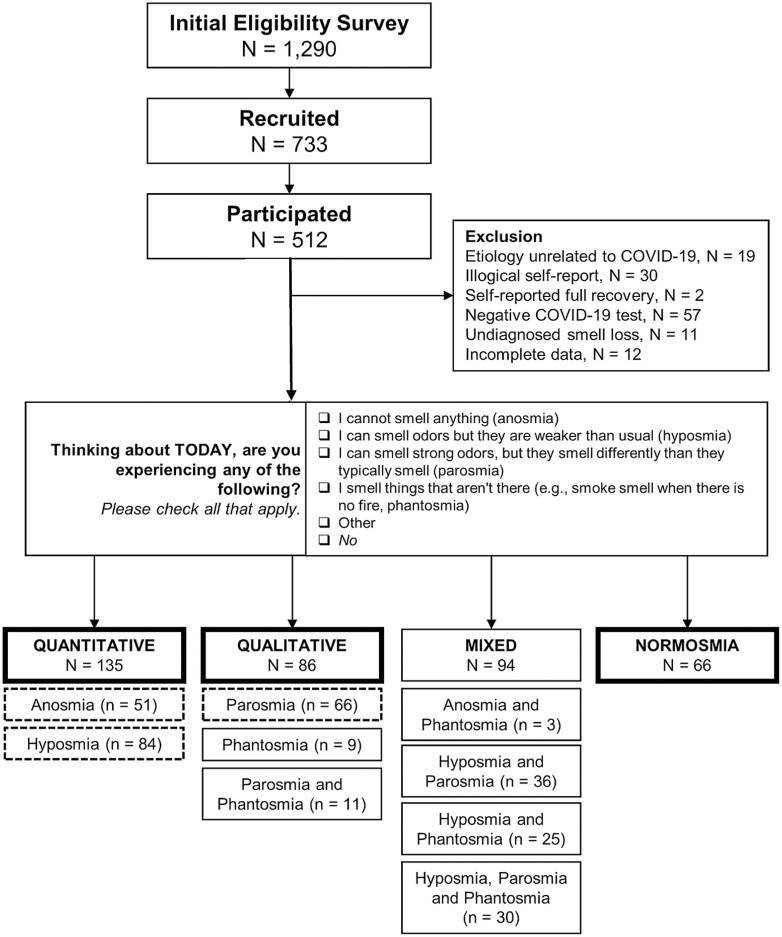
It is estimated that 20%-67% of those with COVID-19 develop olfactory disorders, depending on the SARS-CoV-2 variant. However, there is an absence of quick, population-wide olfactory tests to screen for olfactory disorders. The purpose of this study was to provide a proof-of-concept that SCENTinel 1.1, a rapid, inexpensive, population-wide olfactory test, can discriminate between anosmia (total smell loss), hyposmia (reduced sense of smell), parosmia (distorted odor perception), and phantosmia (odor sensation without a source). Participants were mailed a SCENTinel 1.1 test, which measures odor detection, intensity, identification, and pleasantness, using one of 4 possible odors. Those who completed the test (N = 287) were divided into groups based on their self-reported olfactory function: quantitative olfactory disorder only (anosmia or hyposmia, N = 135), qualitative olfactory disorder only (parosmia and/or phantosmia; N = 86), and normosmia (normal sense of smell; N = 66). SCENTinel 1.1 accurately discriminates quantitative olfactory disorders, qualitative olfactory disorders, and normosmia groups. When olfactory disorders were assessed individually, SCENTinel 1.1 discriminates between hyposmia, parosmia, and anosmia. Participants with parosmia rated common odors less pleasant than those without parosmia. We provide proof-of-concept that SCENTinel 1.1, a rapid smell test, can discriminate quantitative and qualitative olfactory disorders, and is the only direct test to rapidly discriminate parosmia.
Keywords: anosmia; hyposmia; parosmia; phantosmia; prediction; smell test.
© The Author(s) 2023. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Update of
-
Proof-of-concept: SCENTinel 1.1 rapidly discriminates COVID-19 related olfactory disorders.medRxiv [Preprint]. 2022 Nov 8:2022.03.23.22272807. doi: 10.1101/2022.03.23.22272807. medRxiv. 2022. Update in: Chem Senses. 2023 Jan 1;48:bjad002. doi: 10.1093/chemse/bjad002. PMID: 35350197 Free PMC article. Updated. Preprint.
References
-
- Albers MW, Tabert MH, Devanand DP.. Olfactory dysfunction as a predictor of neurodegenerative disease. Curr Neurol Neurosci Rep. 2006;6(5):379–386. - PubMed
-
- Barresi M, Ciurleo R, Giacoppo S, Foti Cuzzola V, Celi D, Bramanti P, Marino S.. Evaluation of olfactory dysfunction in neurodegenerative diseases. J Neurol Sci. 2012;323(1–2):16–24. - PubMed
-
- Bonfils P, Avan P, Faulcon P, Malinvaud D.. Distorted odorant perception: analysis of a series of 56 patients with parosmia. Arch Otolaryngol Head Neck Surg. 2005;131(2):107–112. - PubMed
-
- Bratt M, Skandsen T, Hummel T, Moen KG, Vik A, Nordgård S, Helvik A-S.. Frequency and prognostic factors of olfactory dysfunction after traumatic brain injury. Brain Inj. 2018;32(8):1021–1027. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
