

Performance of standardised colposcopy to detect cervical precancer and cancer for triage of women testing positive for human papillomavirus: results from the ESTAMPA multicentric screening study
- PMID: 36796982
- PMCID: PMC10020136
- DOI: 10.1016/S2214-109X(22)00545-9
Performance of standardised colposcopy to detect cervical precancer and cancer for triage of women testing positive for human papillomavirus: results from the ESTAMPA multicentric screening study
Abstract
Background: Colposcopy, currently included in WHO recommendations as an option to triage human papillomavirus (HPV)-positive women, remains as the reference standard to guide both biopsy for confirmation of cervical precancer and cancer and treatment approaches. We aim to evaluate the performance of colposcopy to detect cervical precancer and cancer for triage in HPV-positive women.
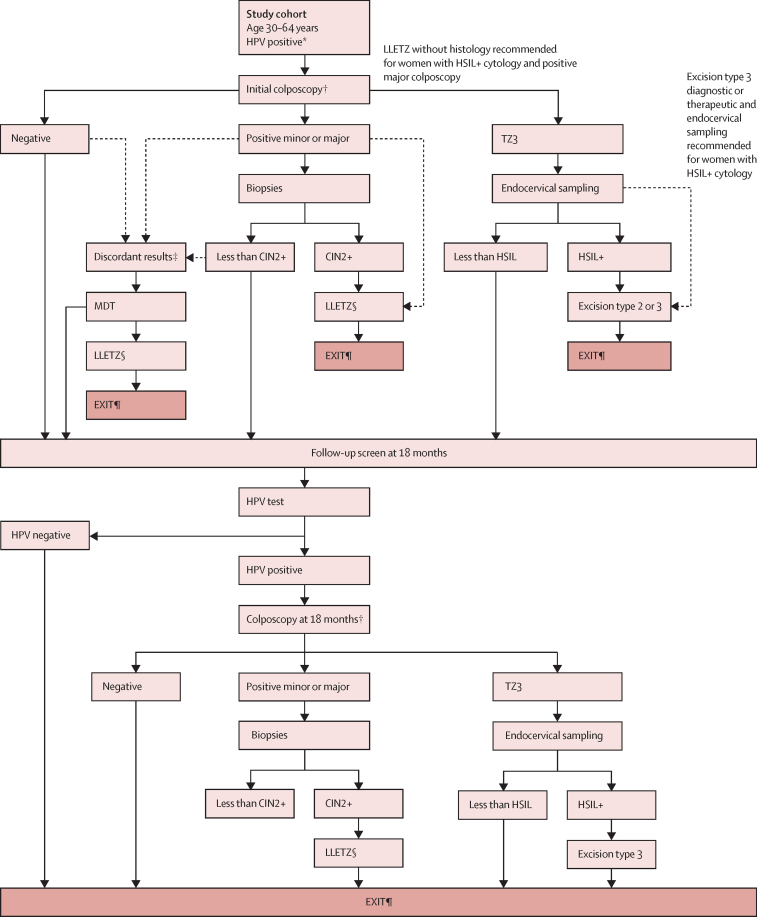
Methods: This cross-sectional, multicentric screening study was conducted at 12 centres (including primary and secondary care centres, hospitals, laboratories, and universities) in Latin America (Argentina, Bolivia, Colombia, Costa Rica, Honduras, Mexico, Paraguay, Peru, and Uruguay). Eligible women were aged 30-64 years, sexually active, did not have a history of cervical cancer or treatment for cervical precancer or a hysterectomy, and were not planning to move outside of the study area. Women were screened with HPV DNA testing and cytology. HPV-positive women were referred to colposcopy using a standardised protocol, including biopsy collection of observed lesions, endocervical sampling for transformation zone (TZ) type 3, and treatment as needed. Women with initial normal colposcopy or no high-grade cervical lesions on histology (less than cervical intraepithelial neoplasia [CIN] grade 2) were recalled after 18 months for another HPV test to complete disease ascertainment; HPV-positive women were referred for a second colposcopy with biopsy and treatment as needed. Diagnostic accuracy of colposcopy was assessed by considering a positive test result when the colposcopic impression at the initial colposcopy was positive minor, positive major, or suspected cancer, and was considered negative otherwise. The main study outcome was histologically confirmed CIN3+ (defined as grade 3 or worse) detected at the initial visit or 18-month visit.
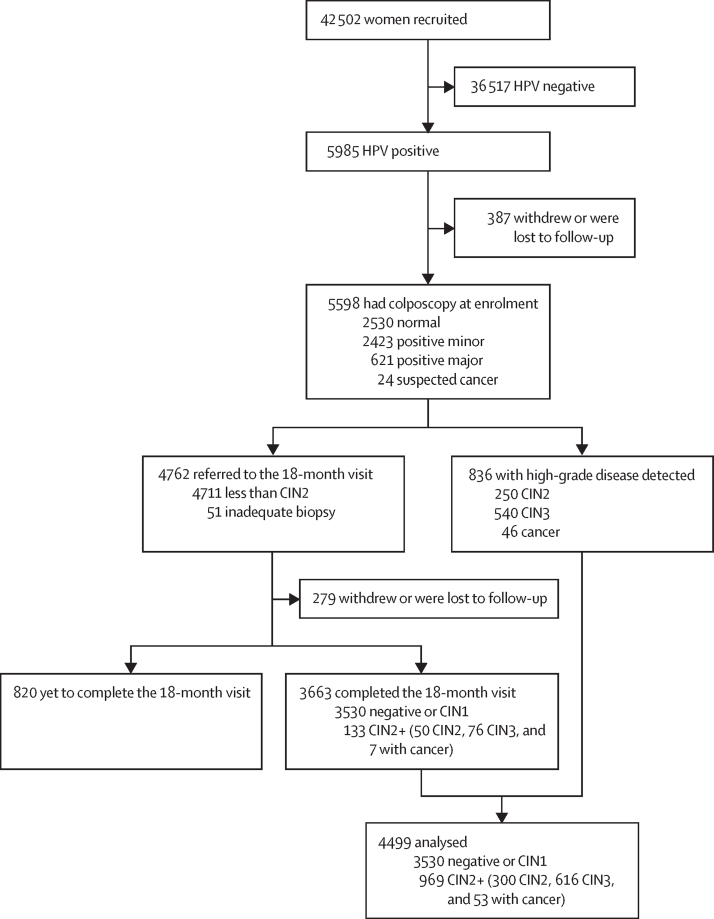
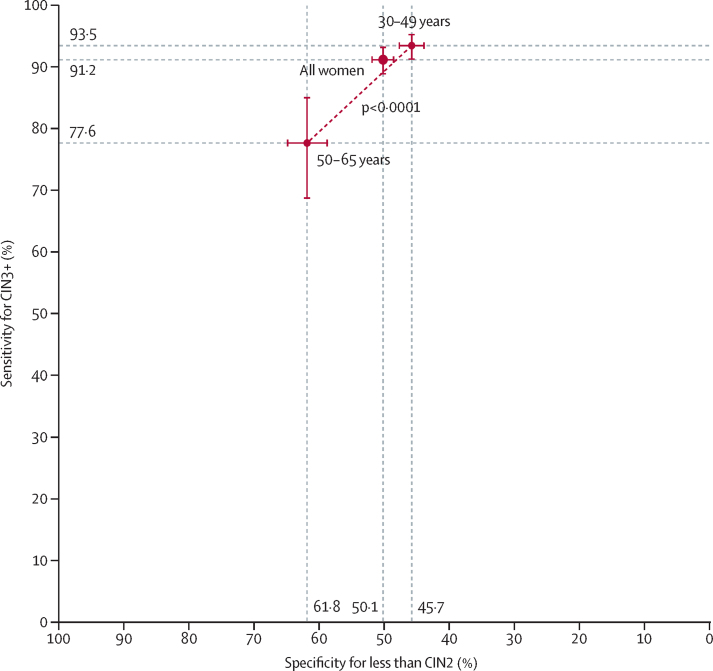
Findings: Between Dec 12, 2012, and Dec 3, 2021, 42 502 women were recruited, and 5985 (14·1%) tested positive for HPV. 4499 participants with complete disease ascertainment and follow-up were included in the analysis, with a median age of 40·6 years (IQR 34·7-49·9). CIN3+ was detected in 669 (14·9%) of 4499 women at the initial visit or 18-month visit (3530 [78·5%] negative or CIN1, 300 [6·7%] CIN2, 616 [13·7%] CIN3, and 53 [1·2%] cancers). Sensitivity was 91·2% (95% CI 88·9-93·2) for CIN3+, whereas specificity was 50·1% (48·5-51·8) for less than CIN2 and 47·1% (45·5-48·7) for less than CIN3. Sensitivity for CIN3+ significantly decreased in older women (93·5% [95% CI 91·3-95·3] in those aged 30-49 years vs 77·6% [68·6-85·0] in those aged 50-65 years; p<0·0001), whereas specificity for less than CIN2 significantly increased (45·7% [43·8-47·6] vs 61·8% [58·7-64·8]; p<0·0001). Sensitivity for CIN3+ was also significantly lower in women with negative cytology than in those with abnormal cytology (p<0·0001).
Interpretation: Colposcopy is accurate for CIN3+ detection in HPV-positive women. These results reflect ESTAMPA efforts in an 18-month follow-up strategy to maximise disease detection with an internationally validated clinical management protocol and regular training, including quality improvement practices. We showed that colposcopy can be optimised with proper standardisation to be used as triage in HPV-positive women.
Funding: WHO; Pan American Health Organization; Union for International Cancer Control; National Cancer Institute (NCI); NCI Center for Global Health; National Agency for the Promotion of Research, Technological Development, and Innovation; NCI of Argentina and Colombia; Caja Costarricense de Seguro Social; National Council for Science and Technology of Paraguay; International Agency for Research on Cancer; and all local collaborative institutions.
© 2023 World Health Organization; licensee Elsevier. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products, or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Conflict of interest statement
Declaration of interests GV reports conference fees from Roche. GIS reports provision of reagents from Roche. CP reports royalties and conferences fees from Roche, MSD, Seegene, Abbot, and Exeltis. TMD reports grants from the US National Cancer Institute, consulting fees from Antiva, and participation on an advisory board for Roche. All other authors declare no competing interests.
Figures
Comment in
-
Colposcopy for cervical screening in low-resource settings.Lancet Glob Health. 2023 Mar;11(3):e304-e305. doi: 10.1016/S2214-109X(23)00014-1. Lancet Glob Health. 2023. PMID: 36796965 No abstract available.
References
-
- Smith HO, Tiffany MF, Qualls CR, Key CR. The rising incidence of adenocarcinoma relative to squamous cell carcinoma of the uterine cervix in the United States—a 24-year population-based study. Gynecol Oncol. 2000;78:97–105. - PubMed
-
- Vaccarella S, Lortet-Tieulent J, Plummer M, Franceschi S, Bray F. Worldwide trends in cervical cancer incidence: impact of screening against changes in disease risk factors. Eur J Cancer. 2013;49:3262–3273. - PubMed
-
- Koss LG. The Papanicolaou test for cervical cancer detection. A triumph and a tragedy. JAMA. 1989;261:737–743. - PubMed
