

Tropifexor for nonalcoholic steatohepatitis: an adaptive, randomized, placebo-controlled phase 2a/b trial
- PMID: 36797481
- PMCID: PMC9941046
- DOI: 10.1038/s41591-022-02200-8
Tropifexor for nonalcoholic steatohepatitis: an adaptive, randomized, placebo-controlled phase 2a/b trial
Abstract
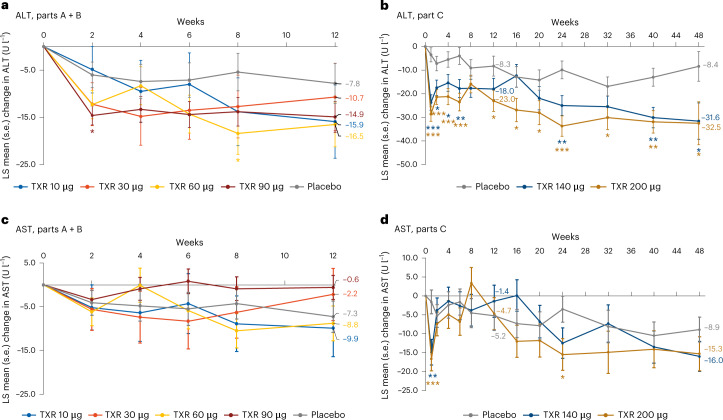
The multimodal activities of farnesoid X receptor (FXR) agonists make this class an attractive option to treat nonalcoholic steatohepatitis. The safety and efficacy of tropifexor, an FXR agonist, in a randomized, multicenter, double-blind, three-part adaptive design, phase 2 study, in patients with nonalcoholic steatohepatitis were therefore assessed. In Parts A + B, 198 patients were randomized to receive tropifexor (10-90 μg) or placebo for 12 weeks. In Part C, 152 patients were randomized to receive tropifexor 140 µg, tropifexor 200 µg or placebo (1:1:1) for 48 weeks. The primary endpoints were safety and tolerability to end-of-study, and dose response on alanine aminotransferase (ALT), aspartate aminotransferase (AST) and hepatic fat fraction (HFF) at week 12. Pruritus was the most common adverse event in all groups, with a higher frequency in the 140- and 200-µg tropifexor groups. Decreases from baseline in ALT and HFF were greater with tropifexor versus placebo at week 12, with a relative decrease in least squares mean from baseline observed with all tropifexor doses for ALT (tropifexor 10-90-μg dose groups ranged from -10.7 to -16.5 U l-1 versus placebo (-7.8 U l-1) and tropifexor 140- and 200-μg groups were -18.0 U l-1 and -23.0 U l-1, respectively, versus placebo (-8.3 U l-1)) and % HFF (tropifexor 10-90-μg dose groups ranged from -7.48% to -15.04% versus placebo (-6.19%) and tropifexor 140- and 200-μg groups were -19.07% and -39.41%, respectively, versus placebo (-10.77%)). Decreases in ALT and HFF were sustained up to week 48; however, similar trends in AST with tropifexor at week 12 were not observed. As with other FXR agonists, dose-related pruritus was frequently observed. Clinicaltrials.gov registration: NCT02855164.
© 2023. The Author(s).
Conflict of interest statement
A.J.S. holds stock options in Exhalenz, Durect, Genfit, Hemoshear, Indalo, Rivus, Sanyal Bio and Tiziana; has received paid consulting advisor fees from Albireo, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Conatus, Covance, Eli Lilly, Genentech, Genfit, Gilead, Hemoshear, HistoIndex, Inventiva, Janssen Pharmaceuticals, Mallinckrodt Pharmaceuticals, Madrigal, Merck, NGM Bio, NorthSea, Novartis, Novo Nordisk, Path AI, Pfizer, Poxel, Prosciento, Regeneron, Roche, Salix, Sanofi, Siemens, Takeda, Terns and 89Bio; is a nonpaid consultant for Amra, Biocellvia, Galectin, Fractyl, Immunron, Intercept and Perspectum; provided consultant advice for AstraZeneca, for which renumeration was paid to Virginia Commonwealth University; was a member of a Data and Safety Monitoring Board for a study funded by Sequana; has received research grants from Boehringer Ingelheim, Bristol Myers Squibb, Conatus, Covance, Eli Lilly, Fractyl, Gilead, Inventiva, Madrigal, Mallinckrodt Pharmaceuticals, Merck, Novartis and Novo Nordisk; has an ongoing research collaboration without direct funding with Echosense-Sandhill, Owl, Second Genome and Siemens; received study drug for the National Institute on Alcohol Abuse and Alcoholism (NIAAA) trial of Imm124 for patients with alcoholic hepatitis from Immuron, without funding; and has received royalties from Elsevier and UpToDate. P.L., J.L., F.S., M.M. and C.A.B. are employees and shareholders of Novartis. E.J.L. received grant/research support from Health, Boehringer Ingelheim, Bristol Myers Squibb, CytoDyn, Durect Corporation, Eli Lilly and Company, Enanta Pharmaceuticals, Galectin Therapeutics, Galmed Pharmaceuticals, Genentech, Gilead Sciences, Hanmi Pharmaceuticals, Intercept Pharmaceuticals, Janssen Pharmaceuticals, the Laboratory for Advanced Medicine, Madrigal Pharmaceuticals, Merck & Co., Metacrine, NGM Biopharmaceuticals Inc., NorthSea Therapeutics, Novartis, Novo Nordisk Inc., Pfizer, Poxel Co., Roche, Sagimet Biosciences, Terns Pharmaceuticals, Valeant Pharmaceuticals, Viking Therapeutics and Zydus Pharmaceuticals. K.J.L., C.S., Y.-C.C., D.A., H.T. and H.H. have nothing to disclose. W.K. served as a speaker and consultant of Boehringer Ingelheim, Novo Nordisk, HK Inoen, Standigm, PharmaKing, KOBIOLABS and Eisai; received grants from Gilead, Novartis, Pfizer, Roche, Springbank, Altimmune, Ildong, GreenCross, Galmed, PharmaEssentia, Dicerna, Celgene and Enyo; and owns stocks in KOBIOLABS and Lepidyne. G.B.B.G. consulted for Gilead, Boehringer Ingelheim and Ionis Pharmaceuticals; and is a speaker for Novo Nordisk and Echosens. J.-F.H. is a consultant for Roche, BMS, Gilead, Merck, Sysmex, PharmaEssentia Pharmaceuticals and Polaris Pharmaceuticals; and is a speaker for AbbVie, BMS, Gilead, Merck, Sysmex, AbbVie and Roche. P.A. is a consultant for Intercept, Gilead, Janssen, Genfit, Boehringer Ingelheim, Falk, Glaxo Smith Kline, Novartis, Genfit, CymaBay and Eiger. S.H.H. received indirect research support from Novartis. V.R. is a consultant for Intercept, Bristol Myers Squibb, Theratechnologie, Poxel, Galmed, ENYO, Novo Nordisk, Boehringer Ingelheim, AstraZeneca, Sagimet and NGM Biopharmaceuticals; and received grant/research support from Gilead and Intercept. A.M.S. received grant/research support from Akero, Bristol Myers Squibb, Boehringer Ingelgeim, Celgene, Gilead, Roche-Genetech, Galectin, Ionis, Intercept, Madrigal, NGM, NorthSea, Novartis, Novo Nordisk and Viking. J. M.V. is a consultant for Arena, Blade, CymaBay, Enanta, Gilead, Intercept, Merck, Novartis and Sundise; received grant/research support from Allergan, Alnyam, 89Bio, Blade, BMS, Celgene, Conatus, CymaBay, Exalenz, Galectin, Galmed, Genfit, Gilead, Hanmi, Icon, Intercept, Merck, Mochida, Molecular Stethoscope, Novartis, Novo Nordisk, Pfizer and Tobira; and is on Data Safety Management Boards for the NIH NIDDK Drug-Induced Liver Injury Network (DILIN) and Fractyl. Y.J.K. received research grant support from BTG, Boston Scientific, AstraZeneca, Gilead Sciences, Samjin and Bayer. D.T. is employed by HistoIndex. Z.G. has no personal conflicts of interest; his institution currently receives funding for research from Novartis, Inventiva, Gilead Sciences, NGM, Bristol Myers Squibb, CymaBay, Eiger, Merck and Intercept. I.R.I.C. and S.L. are former employees and shareholders of Novartis. N.V.N. is a former employee of Novartis.
Figures









Comment in
-
Next-Generation Farnesoid X Receptor Agonists in NASH Treatment: Are We There Yet?Gastroenterology. 2023 Aug;165(2):513-514. doi: 10.1053/j.gastro.2023.03.213. Epub 2023 Mar 21. Gastroenterology. 2023. PMID: 36948425 No abstract available.
-
Tropifexor, a selective non-acid farnesoid X receptor agonist, improved nonalcoholic steatohepatitis in a phase 2 trial, but several issues remain to be resolved.Hepatobiliary Surg Nutr. 2023 Oct 1;12(5):759-762. doi: 10.21037/hbsn-23-342. Epub 2023 Sep 4. Hepatobiliary Surg Nutr. 2023. PMID: 37886193 Free PMC article. No abstract available.
References
-
- European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD) & European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol.64, 1388–1402 (2016). - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
