

This is a preprint.
Derivation and external validation of a clinical prognostic model identifying children at risk of death following presentation for diarrheal care
- PMID: 36798150
- PMCID: PMC9934800
- DOI: 10.1101/2023.02.08.23285625
Derivation and external validation of a clinical prognostic model identifying children at risk of death following presentation for diarrheal care
Update in
-
Derivation and external validation of a clinical prognostic model identifying children at risk of death following presentation for diarrheal care.PLOS Glob Public Health. 2023 Jun 27;3(6):e0001937. doi: 10.1371/journal.pgph.0001937. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37368867 Free PMC article.
Abstract
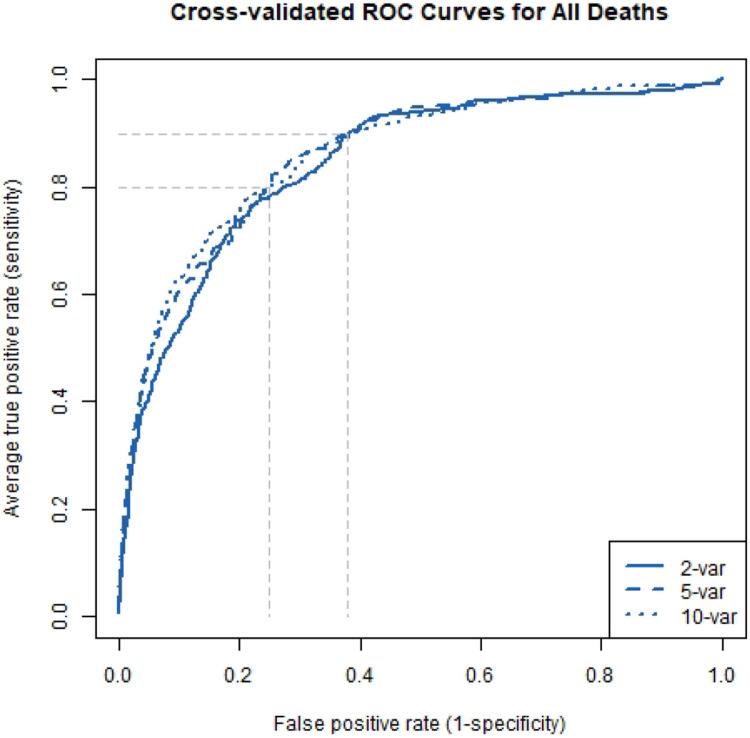
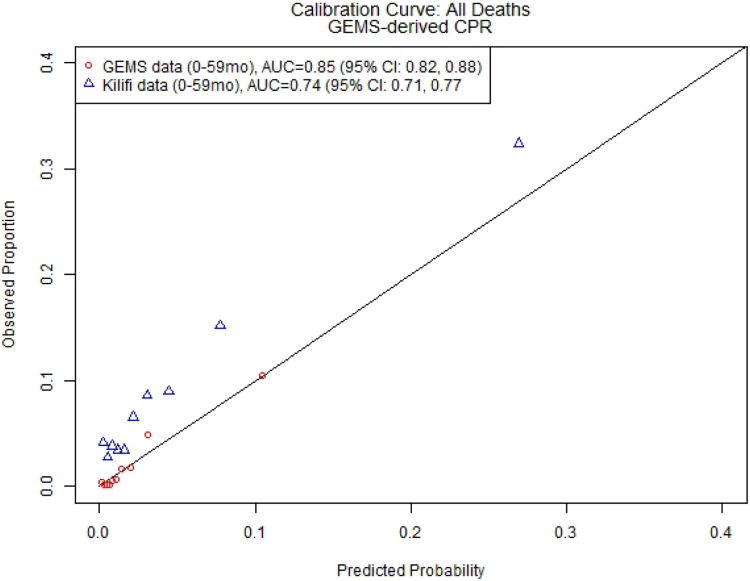
Diarrhea continues to be a leading cause of death for children under-five. Amongst children treated for acute diarrhea, mortality risk remains elevated during and after acute medical management. Identification of those at highest risk would enable better targeting of interventions, but available prognostic tools lack validation. We used clinical and demographic data from the Global Enteric Multicenter Study (GEMS) to build predictive models for death (in-treatment, after discharge, or either) in children aged ≤59 months presenting with moderate-to-severe diarrhea (MSD), in Africa and Asia. We screened variables using random forests, and assessed predictive performance with random forest regression and logistic regression using repeated cross-validation. We used data from the Kilifi Health and Demographic Surveillance System (KHDSS) and Kilifi County Hospital (KCH) in Kenya to externally validate our GEMS-derived clinical prognostic model (CPM). Of 8060 MSD cases, 43 (0.5%) children died in treatment and 122 (1.5% of remaining) died after discharge. MUAC at presentation, respiratory rate, age, temperature, number of days with diarrhea at presentation, number of people living in household, number of children <60 months old living in household, and how much the child had been offered to drink since diarrhea started were predictive of death both in treatment and after discharge. Using a parsimonious 2-variable prediction model, we achieve an AUC=0.84 (95% CI: 0.82, 0.86) in the derivation dataset, and an AUC=0.74 (95% CI 0.71, 0.77) in the external dataset. Our findings suggest it is possible to identify children most likely to die after presenting to care for acute diarrhea. This could represent a novel and cost-effective way to target resources for the prevention of childhood mortality.
Figures
References
-
- Veirum J.E., et al., Increased mortality in the year following discharge from a paediatric ward in Bissau, Guinea-Bissau. Acta Paediatr, 2007. 96(12): p. 1832–8. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources