

This is a preprint.
Clinical testing of transcriptome-wide expression profiles in high-risk localized and metastatic prostate cancer starting androgen deprivation therapy: an ancillary study of the STAMPEDE abiraterone Phase 3 trial
- PMID: 36798177
- PMCID: PMC9934744
- DOI: 10.21203/rs.3.rs-2488586/v1
Clinical testing of transcriptome-wide expression profiles in high-risk localized and metastatic prostate cancer starting androgen deprivation therapy: an ancillary study of the STAMPEDE abiraterone Phase 3 trial
Abstract
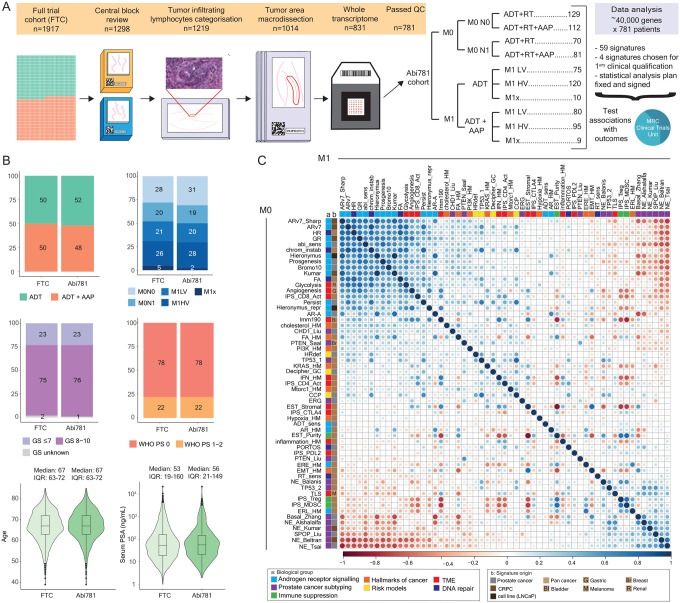
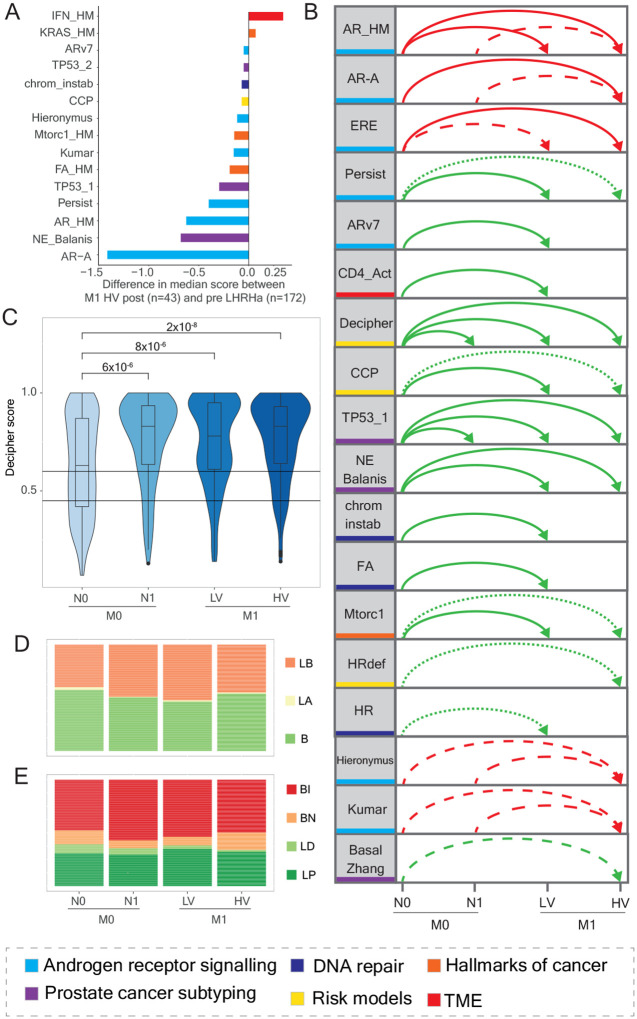
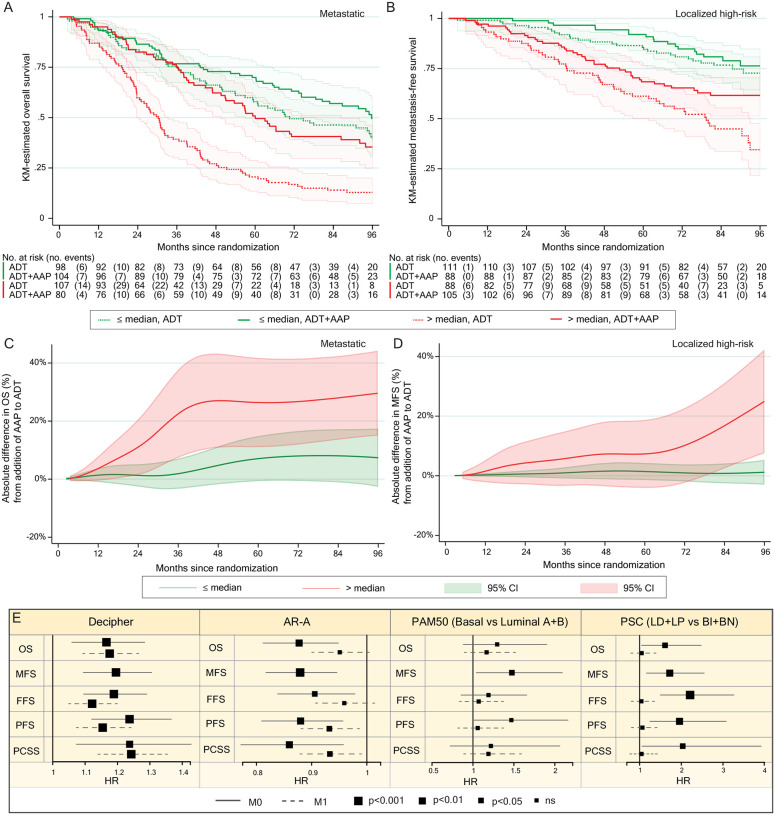
Metastatic and high-risk localized prostate cancer respond to hormone therapy but outcomes vary. Following a pre-specified statistical plan, we used Cox models adjusted for clinical variables to test associations with survival of multi-gene expression-based classifiers from 781 patients randomized to androgen deprivation with or without abiraterone in the STAMPEDE trial. Decipher score was strongly prognostic (p<2×10-5) and identified clinically-relevant differences in absolute benefit, especially for localized cancers. In metastatic disease, classifiers of proliferation, PTEN or TP53 loss and treatment-persistent cells were prognostic. In localized disease, androgen receptor activity was protective whilst interferon signaling (that strongly associated with tumor lymphocyte infiltration) was detrimental. Post-Operative Radiation-Therapy Outcomes Score was prognostic in localized but not metastatic disease (interaction p=0.0001) suggesting the impact of tumor biology on clinical outcome is context-dependent on metastatic state. Transcriptome-wide testing has clinical utility for advanced prostate cancer and identified worse outcomes for localized cancers with tumor-promoting inflammation.
Keywords: Decipher score; Prostate cancer; STAMPEDE trial; high-risk localized; interferon signalling; mRNA; prognosis; synchronous metastatic; transcriptome-wide profiling.
Conflict of interest statement
All other authors declare no competing interests.
Figures

References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
