

Preoperative prognostic prediction for stage I lung adenocarcinomas: Impact of the computed tomography features associated with the new histological grading system
- PMID: 36798818
- PMCID: PMC9927203
- DOI: 10.3389/fonc.2023.1103269
Preoperative prognostic prediction for stage I lung adenocarcinomas: Impact of the computed tomography features associated with the new histological grading system
Abstract
Objectives: This study aimed to identify the computed tomography (CT) features associated with the new International Association for the Study of Lung Cancer (IASLC) three-tiered grading system to improve the preoperative prediction of disease-free survival of stage I lung adenocarcinoma patients.
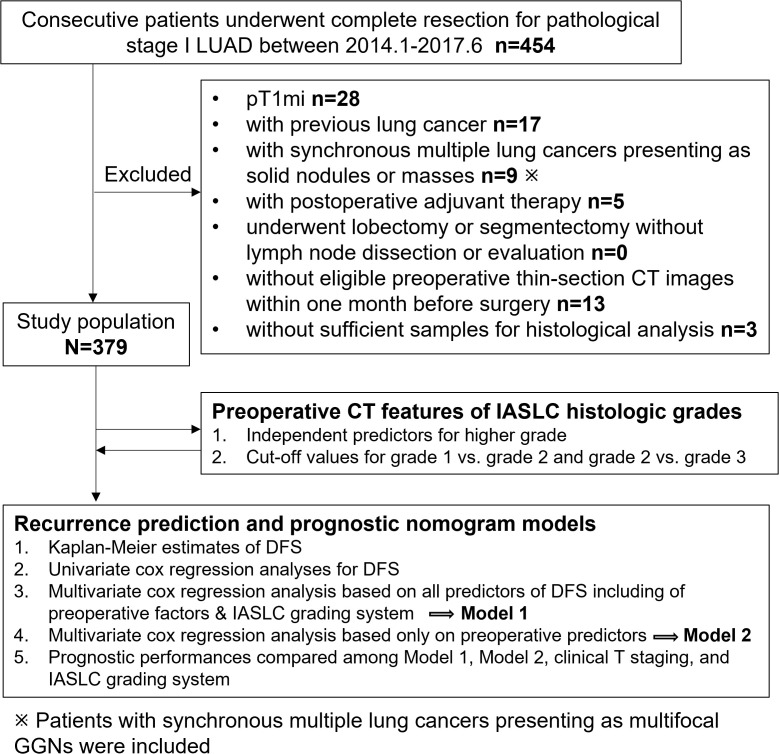
Methods: The study included 379 patients. Ordinal logistic regression analysis was used to identify the independent predictors of IASLC grades. The first multivariate Cox regression model (Model 1) was based on the significant factors from the univariate analysis. The second multivariate model (Model 2) excluded the histologic grade and based only on preoperative factors.
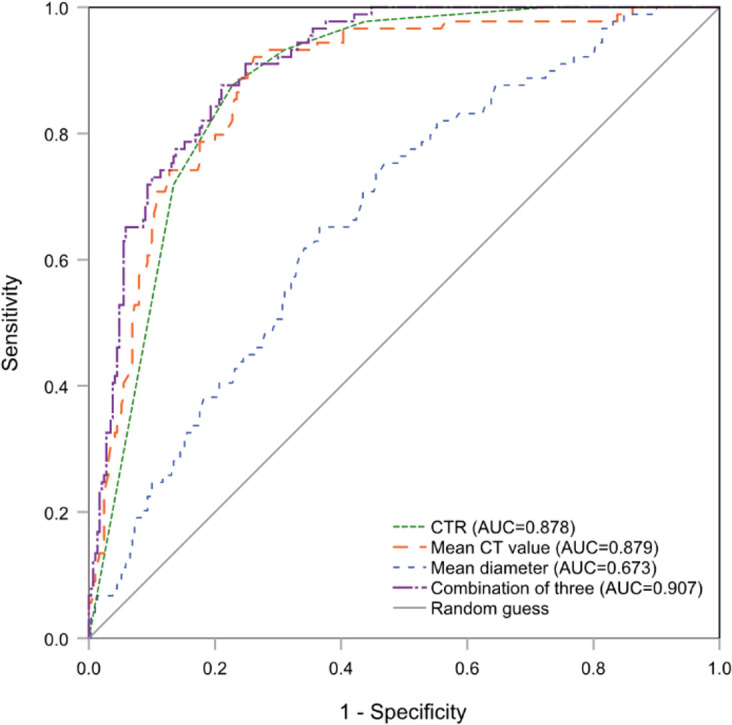
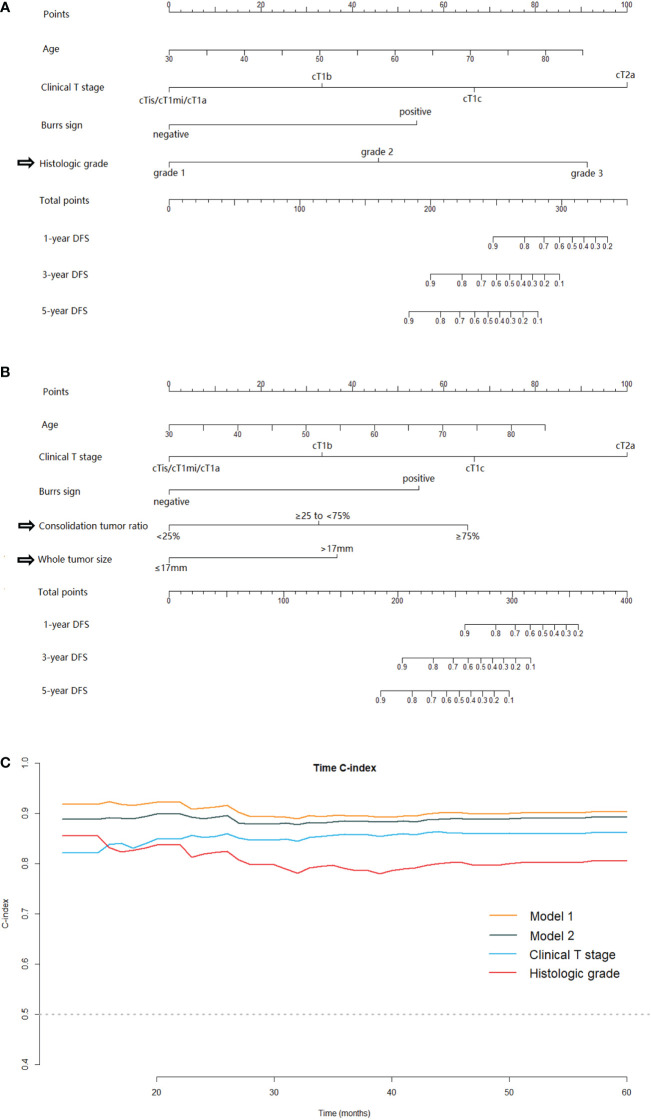
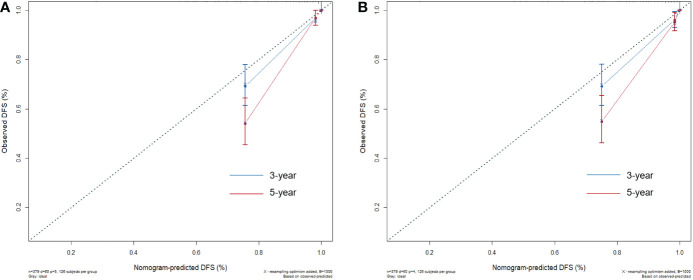
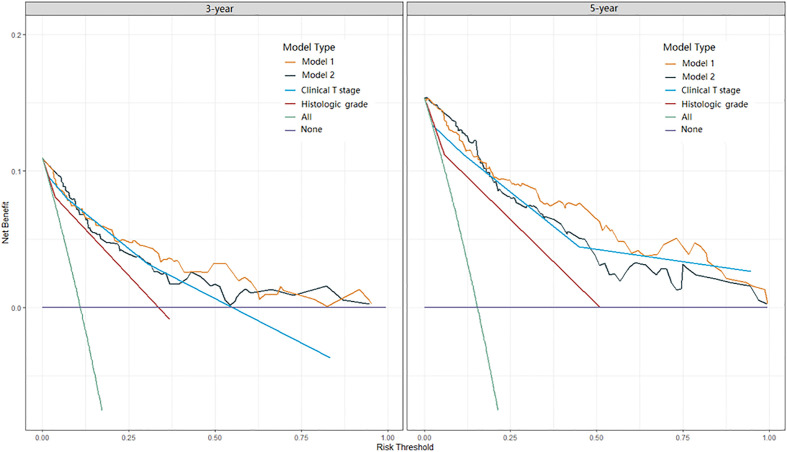
Results: Larger consolidation tumor ratio (OR=2.15, P<.001), whole tumor size (OR=1.74, P=.002), and higher CT value (OR=3.77, P=.001) were independent predictors of higher IASLC grade. Sixty patients experienced recurrences after 70.4 months of follow-up. Model 1 consisted of age (HR:1.05, P=.003), clinical T stage (HR:2.32, P<.001), histologic grade (HR:4.31, P<.001), and burrs sign (HR:5.96, P<.001). Model 2 consisted of age (HR,1.04; P=.015), clinical T stage (HR:2.49, P<.001), consolidation tumor ratio (HR:2.49, P=.016), whole tumor size (HR:2.81, P=.022), and the burrs sign (HR:4.55, P=.002). Model 1 had the best prognostic predictive performance, followed by Model 2, clinical T stage, and histologic grade.
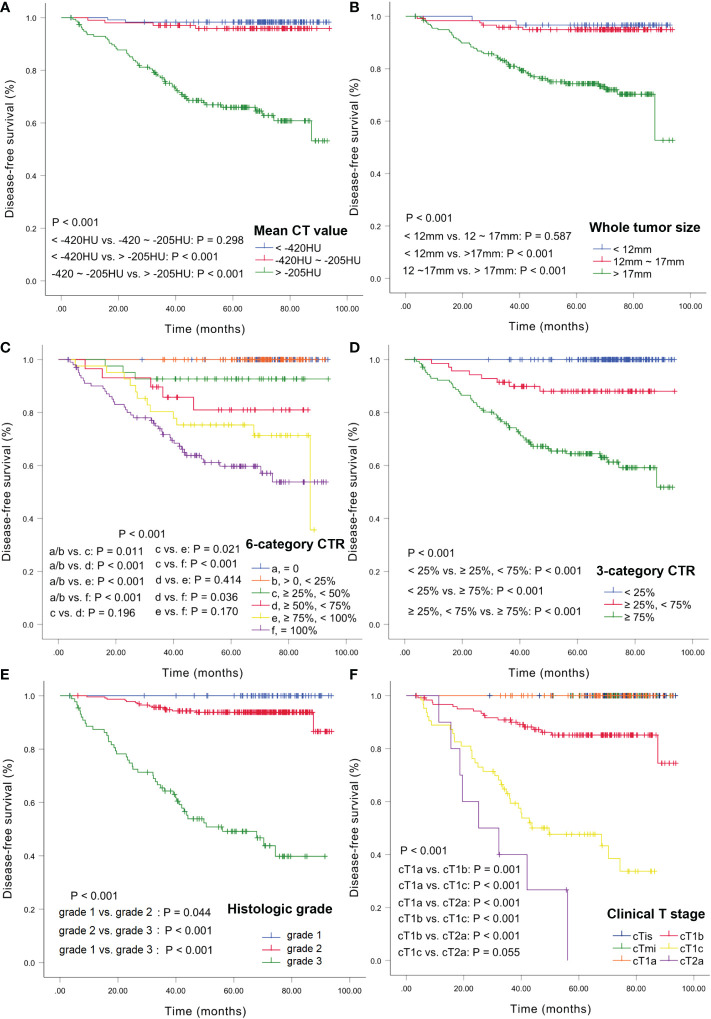
Conclusion: CTR (cut-off values of <25% and ≥75%) and whole tumor size (cut-off value of 17 mm) could stratify patients into different prognosis and be used as preoperative surrogates for the IASLC grading system. Integrating these CT features with clinical T staging can improve the preoperative prognostic prediction for stage I lung adenocarcinoma patients.
Keywords: IASLC grading system; clinical T stage; invasive lung adenocarcinoma; preoperative CT imaging; prognostic model.
Copyright © 2023 Liang, Tang, Tan, Zeng, Guo, Feng and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Application and progress of non-invasive imaging in predicting lung invasive non-mucinous adenocarcinoma under the new IASLC grading guidelines.Insights Imaging. 2025 Jan 2;16(1):4. doi: 10.1186/s13244-024-01877-4. Insights Imaging. 2025. PMID: 39747759 Free PMC article. Review.
-
Clinical implication of the 2020 International Association for the Study of Lung Cancer histologic grading in surgically resected pathologic stage 1 lung adenocarcinomas: Prognostic value and association with computed tomography characteristics.Lung Cancer. 2023 Oct;184:107345. doi: 10.1016/j.lungcan.2023.107345. Epub 2023 Aug 12. Lung Cancer. 2023. PMID: 37611496
-
Added prognostic value of CT characteristics and IASLC/ATS/ERS histologic subtype in surgically resected lung adenocarcinomas.Lung Cancer. 2018 Jun;120:130-136. doi: 10.1016/j.lungcan.2018.04.007. Epub 2018 Apr 11. Lung Cancer. 2018. PMID: 29748007
-
Validation Study of New IASLC Histology Grading System in Stage I Non-Mucinous Adenocarcinoma Comparing With Minimally Invasive Adenocarcinoma.Clin Lung Cancer. 2022 Nov;23(7):e435-e442. doi: 10.1016/j.cllc.2022.06.004. Epub 2022 Jun 22. Clin Lung Cancer. 2022. PMID: 35945128
-
Prognostic impact of the IASLC grading system of lung adenocarcinoma: a systematic review and meta-analysis.Histopathology. 2024 Jul;85(1):51-61. doi: 10.1111/his.15172. Epub 2024 Mar 14. Histopathology. 2024. PMID: 38485464
Cited by
-
Using the length of pleural tag to predetermine pleural invasion by lung adenocarcinomas.Front Oncol. 2024 Nov 1;14:1463568. doi: 10.3389/fonc.2024.1463568. eCollection 2024. Front Oncol. 2024. PMID: 39555451 Free PMC article.
-
CT radiomics from intratumor and peritumor regions for predicting poorly differentiated invasive nonmucinous pulmonary adenocarcinoma.Sci Rep. 2025 Apr 25;15(1):14434. doi: 10.1038/s41598-025-99465-z. Sci Rep. 2025. PMID: 40281090 Free PMC article.
-
Application and progress of non-invasive imaging in predicting lung invasive non-mucinous adenocarcinoma under the new IASLC grading guidelines.Insights Imaging. 2025 Jan 2;16(1):4. doi: 10.1186/s13244-024-01877-4. Insights Imaging. 2025. PMID: 39747759 Free PMC article. Review.
References
-
- Kris MG, Gaspar LE, Chaft JE, Kennedy EB, Azzoli CG, Ellis PM, et al. . Adjuvant systemic therapy and adjuvant radiation therapy for stage I to IIIA completely resected non-Small-Cell lung cancers: American society of clinical Oncology/Cancer care Ontario clinical practice guideline update. J Clin Oncol (2017) 35:2960–74. doi: 10.1200/jco.2017.72.4401 - DOI - PubMed
-
- Okami J, Shintani Y, Okumura M, Ito H, Ohtsuka T, Toyooka S, et al. . Demographics, safety and quality, and prognostic information in both the seventh and eighth editions of the TNM classification in 18,973 surgical cases of the Japanese joint committee of lung cancer registry database in 2010. J Thorac Oncol (2019) 14:212–22. doi: 10.1016/j.jtho.2018.10.002 - DOI - PubMed
LinkOut - more resources
Full Text Sources