

Transcatheter Electrosurgery: A Narrative Review
- PMID: 36799217
- PMCID: PMC10108249
- DOI: 10.1161/CIRCINTERVENTIONS.122.012019
Transcatheter Electrosurgery: A Narrative Review
Abstract
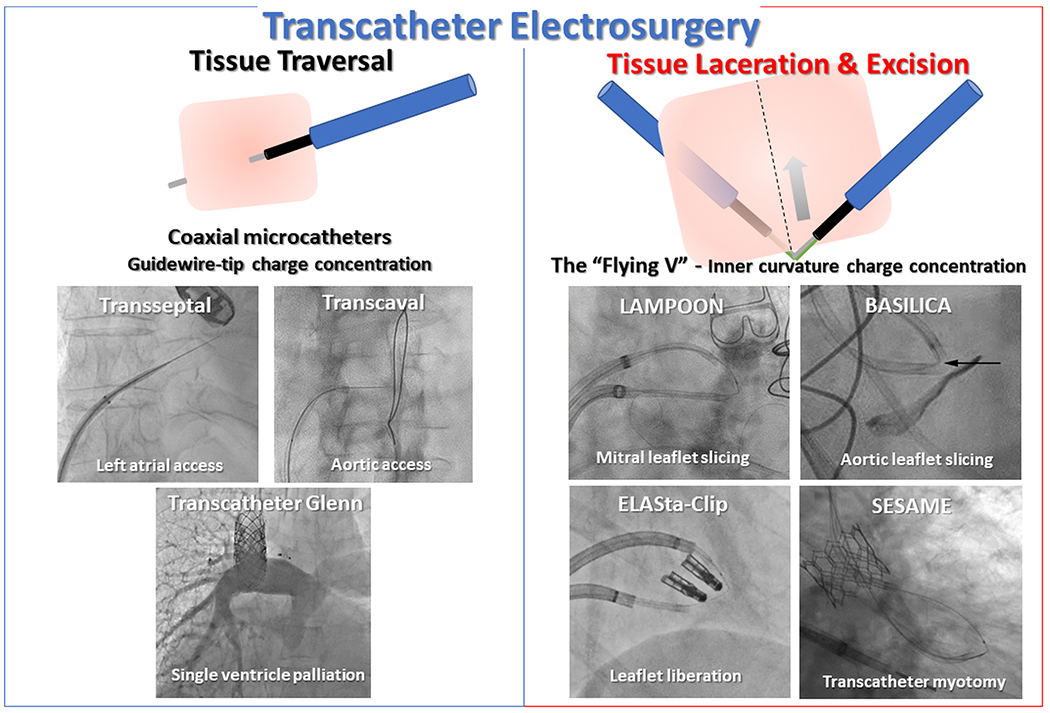
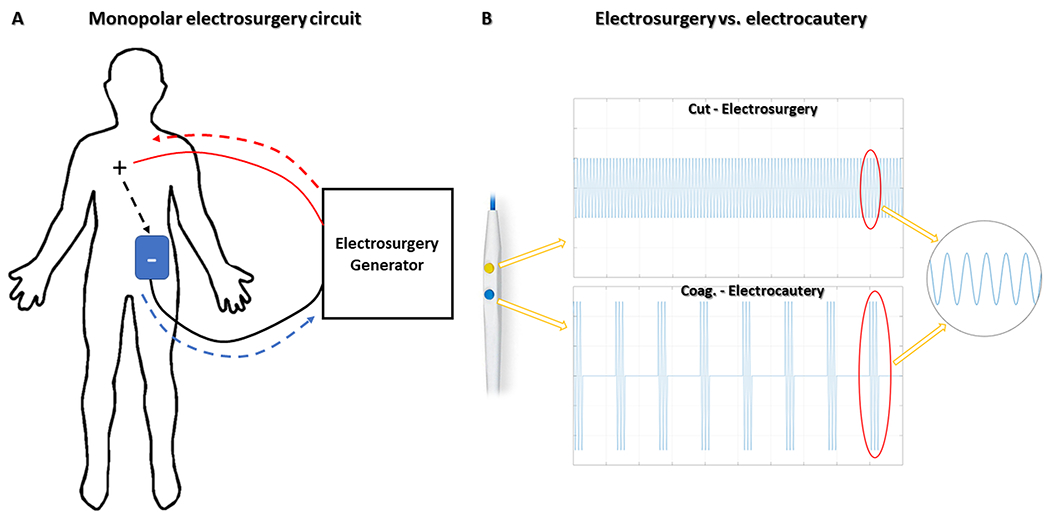
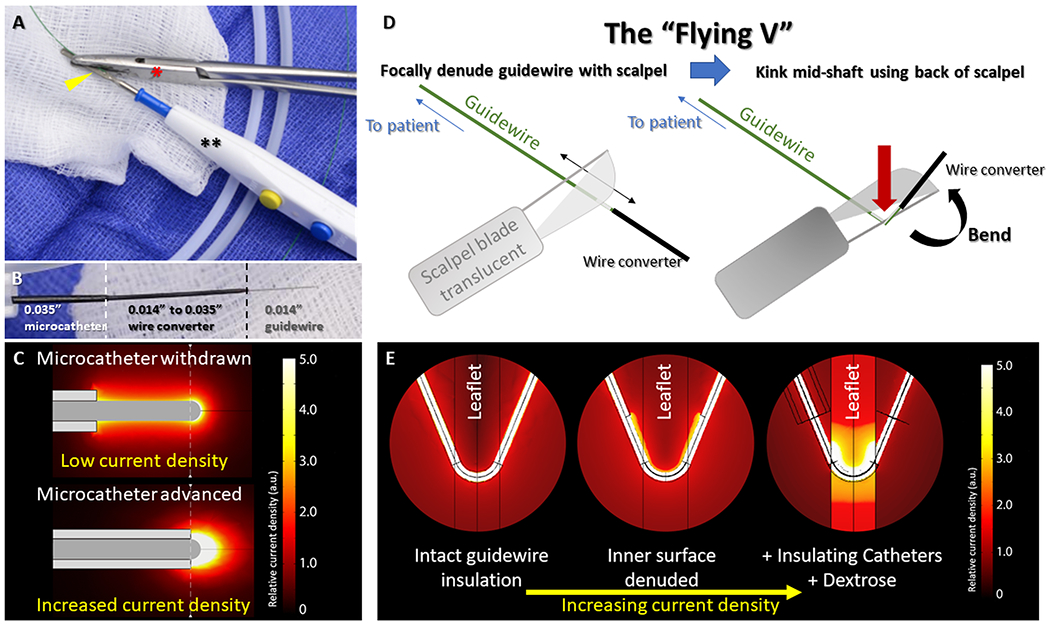
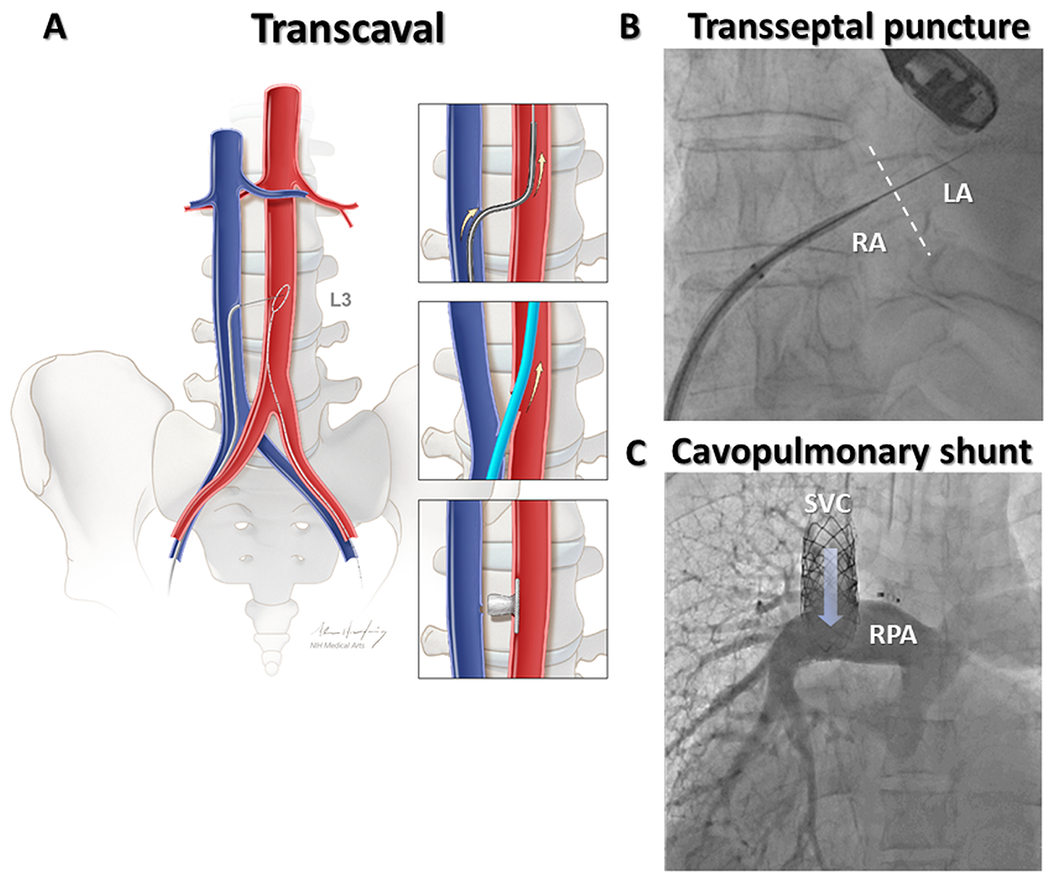
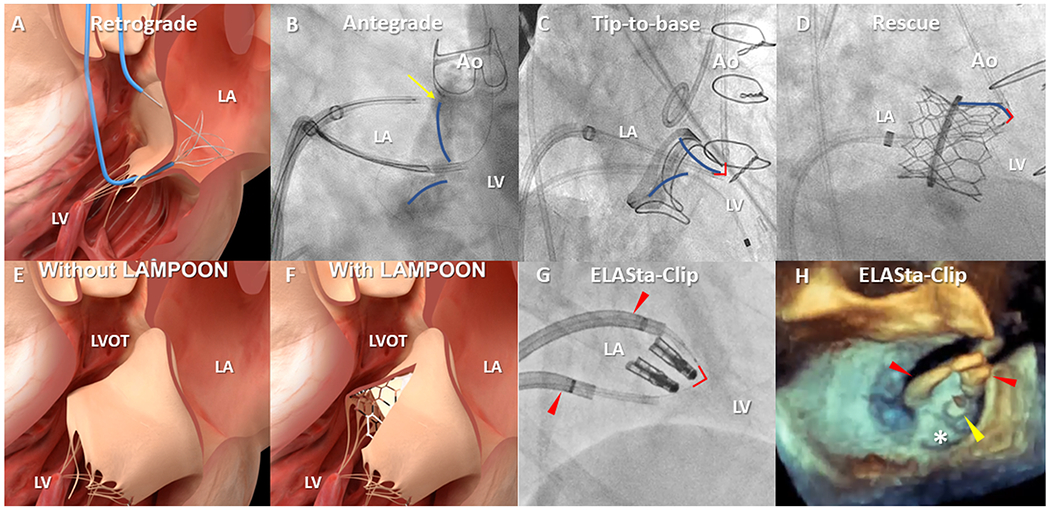
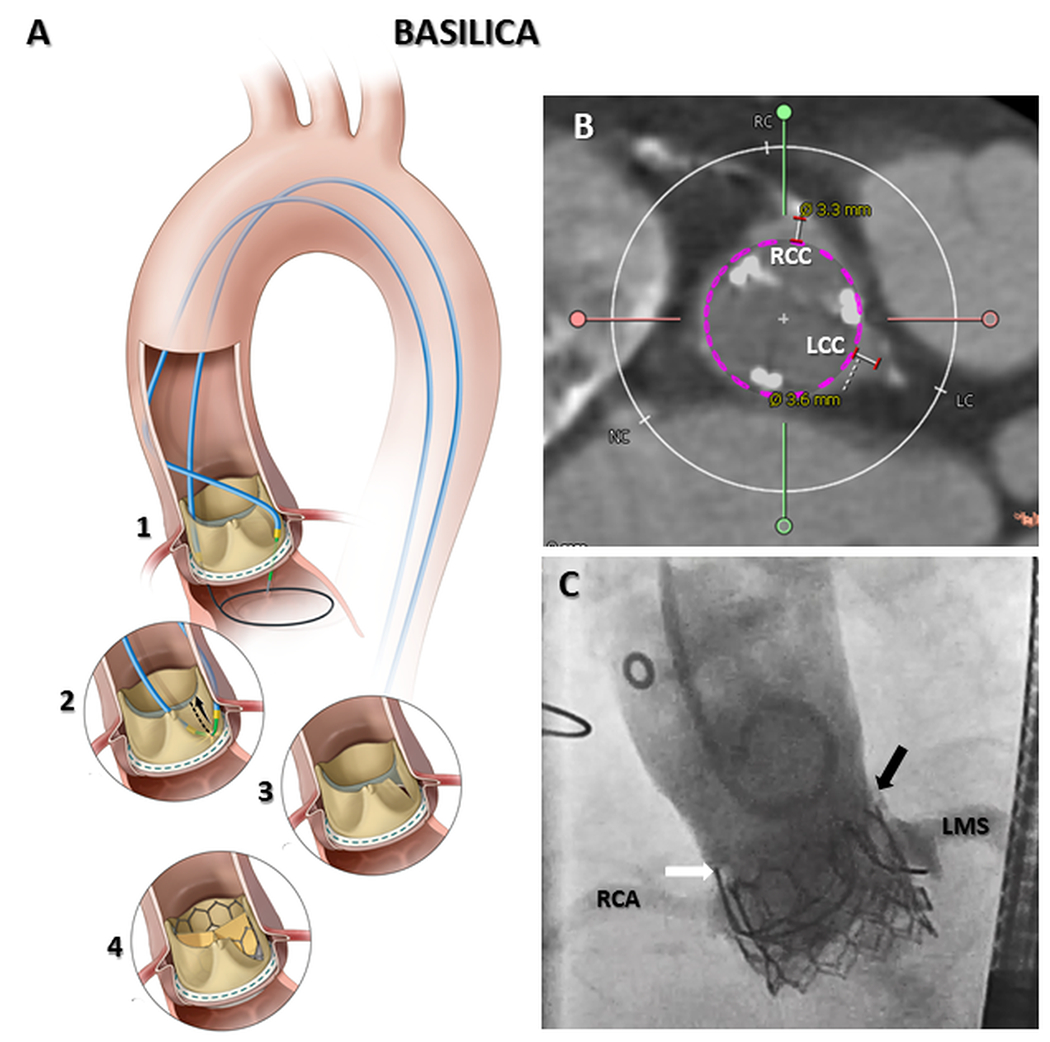
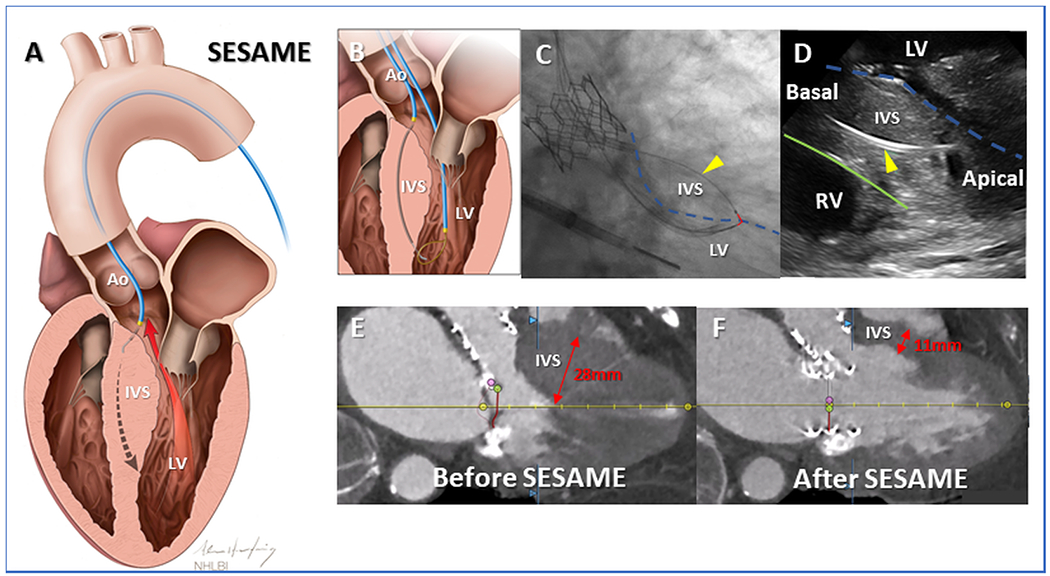
Transcatheter electrosurgery describes the ability to cut and traverse tissue, at a distance, without an open surgical field and is possible using either purpose-built or off-the-shelf devices. Tissue traversal requires focused delivery of radiofrequency energy to a guidewire tip. Initially employed to cross atretic pulmonary valves, tissue traversal has enabled transcaval aortic access, recanalization of arterial and venous occlusions, transseptal access, and many other techniques. To cut tissue, the selectively denuded inner curvature of a kinked guidewire (the Flying-V) or a single-loop snare is energized during traction. Adjunctive techniques may complement or enable contemporary transcatheter procedures, whereas myocardial slicing or excision of ectopic masses may offer definitive therapy. In this contemporary review we discuss the principles of transcatheter electrosurgery, and through exemplary clinical applications highlight the range of therapeutic options offered by this versatile family of procedures.
Keywords: catheter; catheterization; electrode; electrosurgery; transcatheter aortic valve replacement.
Figures
References
-
- Akagi T, Hashino K, Maeno Y, Ishii M, Sugimura T, Kawano T, Kato H. Balloon dilatation of the pulmonary valve in a patient with pulmonary atresia and intact ventricular septum using a commercially available radiofrequency catheter. Pediatr Cardiol. 1997;18:61–63. doi: 10.1007/s002469900112 - DOI - PubMed
-
- Alwi M, Geetha K, Bilkis AA, Lim MK, Hasri S, Haifa AL, Sallehudin A, Zambahari R. Pulmonary atresia with intact ventricular septum percutaneous radiofrequency-assisted valvotomy and balloon dilation versus surgical valvotomy and Blalock Taussig shunt. J Am Coll Cardiol. 2000;35:468–476. doi: 10.1016/s0735-1097(99)00549-5 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
