

Association of admission frailty and frailty changes during cardiac rehabilitation with 5-year outcomes
- PMID: 36799963
- PMCID: PMC10335868
- DOI: 10.1093/eurjpc/zwad048
Association of admission frailty and frailty changes during cardiac rehabilitation with 5-year outcomes
Abstract
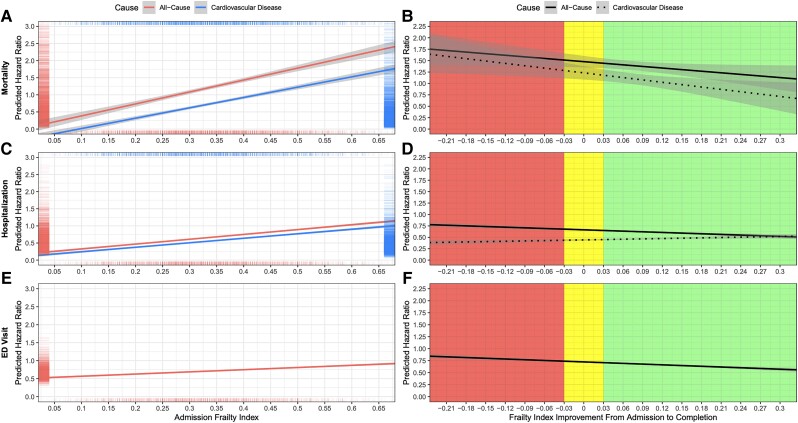
Aims: Examine the association between (1) admission frailty and (2) frailty changes during cardiac rehabilitation (CR) with 5-year outcomes (i.e. time to mortality, first hospitalization, first emergency department (ED) visit, and number of hospitalizations, hospital days, and ED visits).
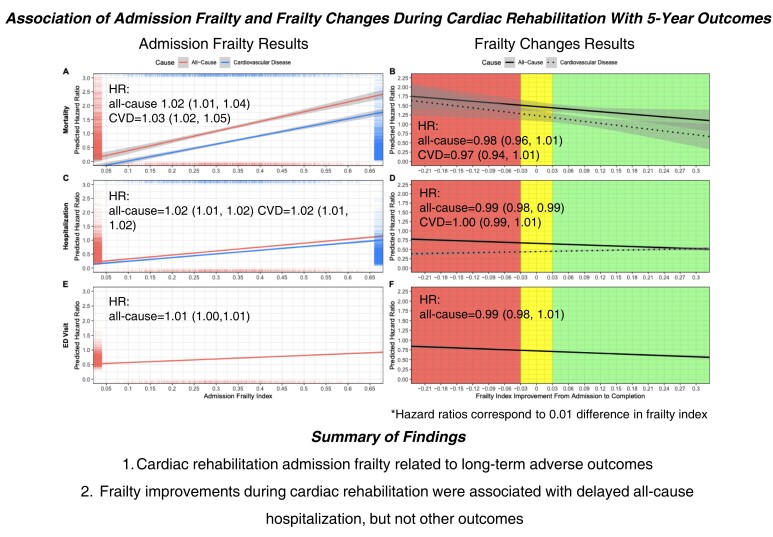
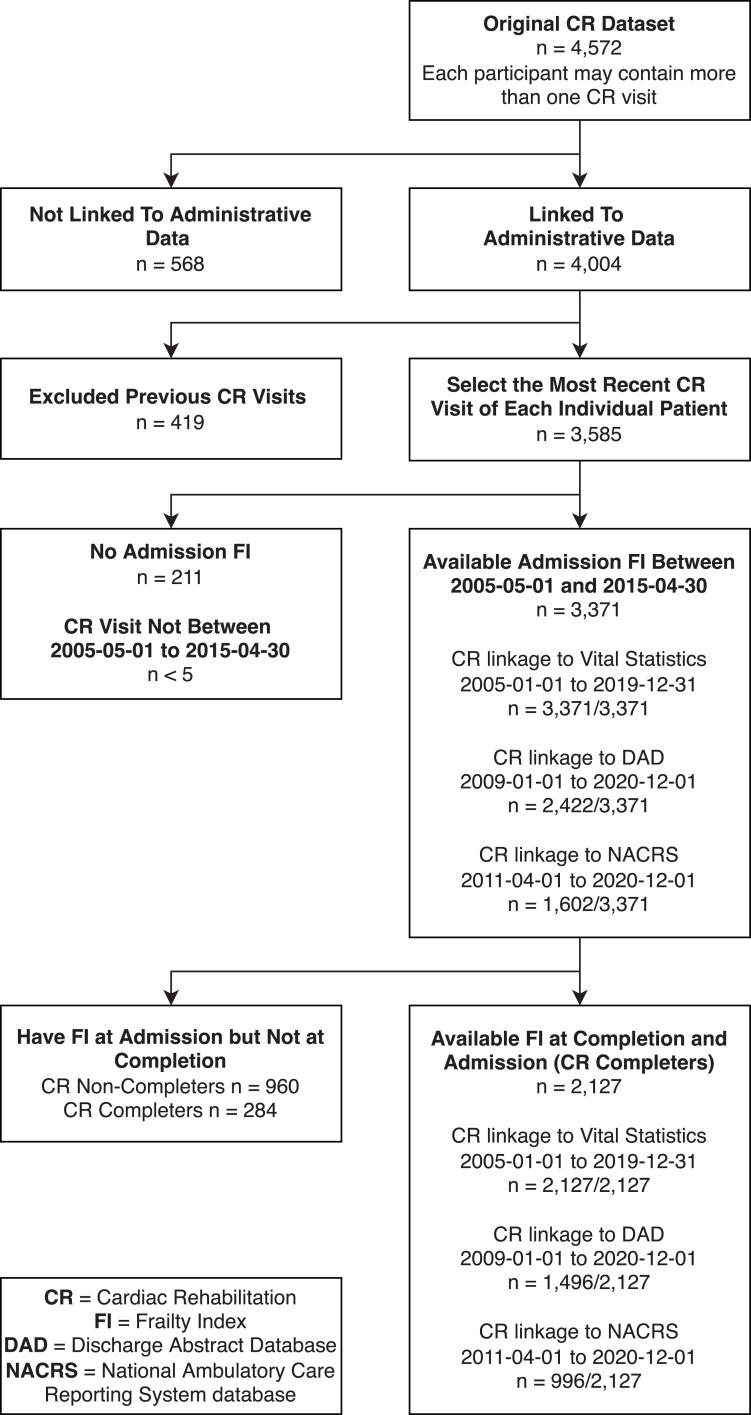
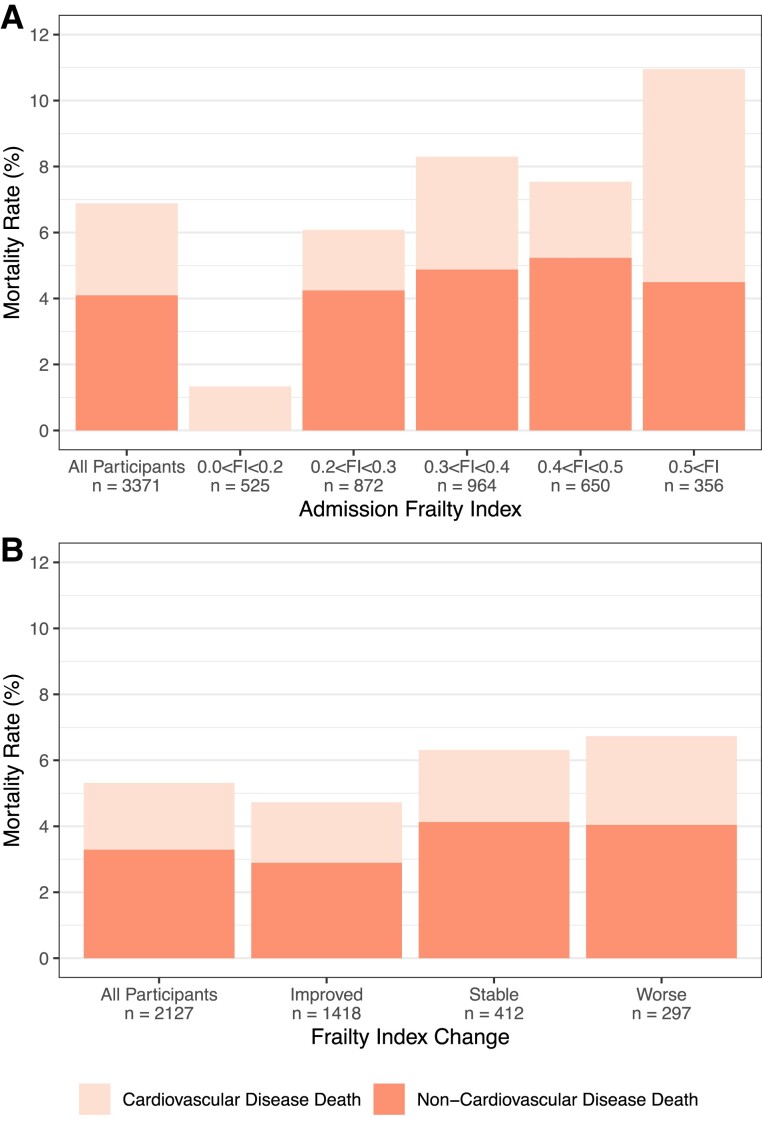
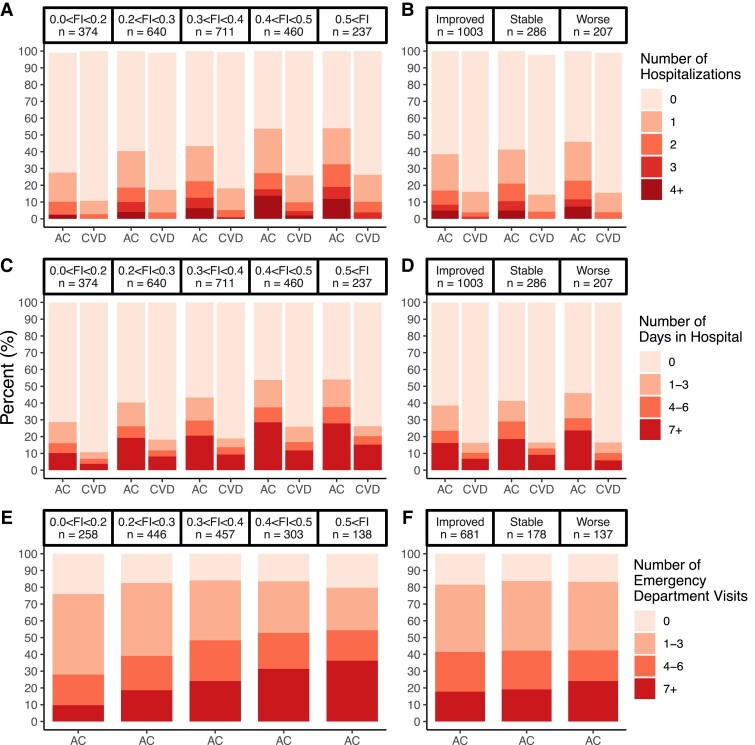
Methods and results: Data from patients admitted to a 12-week CR programme in Halifax, Nova Scotia, from May 2005 to April 2015 (n = 3371) were analysed. A 25-item frailty index (FI) estimated frailty levels at CR admission and completion. FI improvements were determined by calculating the difference between admission and discharge FI. CR data were linked to administrative health data to examine 5-year outcomes [due to all causes and cardiovascular diseases (CVDs)]. Cox regression, Fine-Gray models, and negative binomial hurdle models were used to determine the association between FI and outcomes. On average, patients were 61.9 (SD: 10.7) years old and 74% were male. Mean admission FI scores were 0.34 (SD: 0.13), which improved by 0.07 (SD: 0.09) by CR completion. Admission FI was associated with time to mortality [HRs/IRRs per 0.01 FI increase: all causes = 1.02(95% CI 1.01,1.04); CVD = 1.03(1.02,1.05)], hospitalization [all causes = 1.02(1.01,1.02); CVD = 1.02(1.01,1.02)], ED visit [all causes = 1.01(1.00,1.01)], and the number of hospitalizations [all causes = 1.02(95% CI 1.01,1.03); CVD = 1.02(1.00,1.04)], hospital days [all causes = 1.01(1.01,1.03)], and ED visits [all causes = 1.02(1.02,1.03)]. FI improvements during CR had a protective effect regarding time to all-cause hospitalization [0.99(0.98,0.99)] but were not associated with other outcomes.
Conclusion: Frailty status at CR admission was related to long-term adverse outcomes. Frailty improvements during CR were associated with delayed all-cause hospitalization, in which a larger effect was associated with a greater chance of improved outcome.
Keywords: Cardiac rehabilitation; Frailty; Hospitalization; Mortality.
Plain language summary
This work improves our understanding of the relationship between admission frailty and frailty changes with mortality, hospitalization, and emergency department (ED) use in a cardiac rehabilitation (CR) setting. Frailty changes during CR were related with time to hospitalization due to any cause.Higher frailty levels at admission of CR were related to lower time to death, re-hospitalization, and ED visit and to a higher total number of hospitalizations and ED visits due to all causes or due to cardiovascular diseases.Overall, this work underscores the importance of considering the degree of frailty in the CR setting for the purpose of predicting adverse outcomes.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: J.Q., D.S.K., N.G., C.M., C.B., OT, and W.F.: none; K.R. has asserted copyright of the Clinical Frailty Scale through Dalhousie University’s Industry, Liaison, and Innovation Office. Use is free for education, research, and not-for-profit health care. Users agree not to change or commercialize the scale. In addition to academic and hospital appointments, K.R. is cofounder of Ardea Outcomes, which (as DGI Clinical) in the last 3 years has contracts with pharma and device manufacturers (Biogen, Hollister, INmune, Novartis, Nutricia, and Takeda) on individualized outcome measurement. In 2019, K.R. was paid an honorarium for an interview with Biogen. In 2020, he attended an advisory board meeting with Nutricia on dementia and chaired a scientific workshop and technical review panel on frailty for the Singapore National Research Foundation. Otherwise, any personal fees were for invited guest lectures, rounds, and academic symposia, received directly from event organizers for presentations on frailty. K.R. is an associate director of the Canadian Consortium on Neurodegeneration in Aging, which is funded by the Canadian Institutes for Health Research, the Alzheimer Society of Canada, and several other charities.
Figures
Comment in
-
The many uses of frailty assessments in cardiac rehabilitation programs.Eur J Prev Cardiol. 2023 Jul 12;30(9):805-806. doi: 10.1093/eurjpc/zwad065. Eur J Prev Cardiol. 2023. PMID: 36857614 No abstract available.
References
-
- World Health Organization . Cardiovascular Diseases (CVDs): Geneva, Switzerland. World Health Organization; 2021.
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, Elkind MSV, Evenson KR, Ferguson JF, Gupta DK, Khan SS, Kissela BM, Knutson KL, Lee CD, Lewis TT, Liu J, Loop MS, Lutsey PL, Ma J, Mackey J, Martin SS, Matchar DB, Mussolino ME, Navaneethan SD, Perak AM, Roth GA, Samad Z, Satou GM, Schroeder EB, Shah SH, Shay CM, Stokes A, VanWagner LB, Wang NY, Tsao CW. . Heart disease and stroke statistics—2021 update. Circulation 2021;143:e254–e743. - PubMed
-
- Leal J, Luengo-Fernández R, Gray A, Petersen S, Rayner M. Economic burden of cardiovascular diseases in the enlarged European Union. Eur Heart J 2006;27:1610–1619. - PubMed
-
- Kanasi E, Ayilavarapu S, Jones J. The aging population: demographics and the biology of aging. Periodontol 2000 2016;72:13–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
