

Clinical Presentations of Drug-Induced Hyperprolactinaemia: A Literature Review
- PMID: 36800148
- PMCID: PMC10097739
- DOI: 10.1007/s40290-023-00462-2
Clinical Presentations of Drug-Induced Hyperprolactinaemia: A Literature Review
Abstract
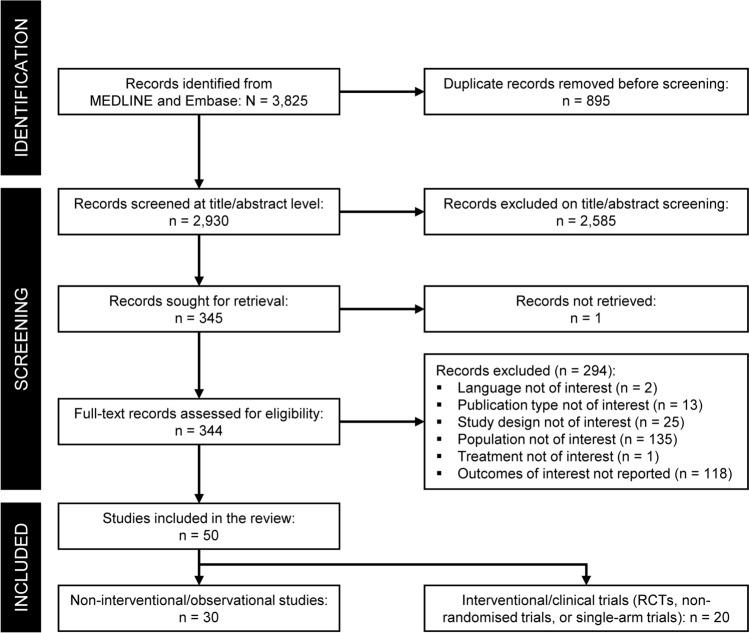
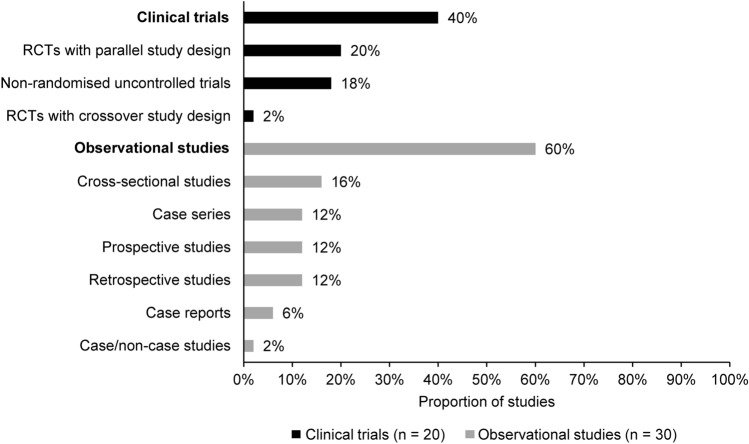
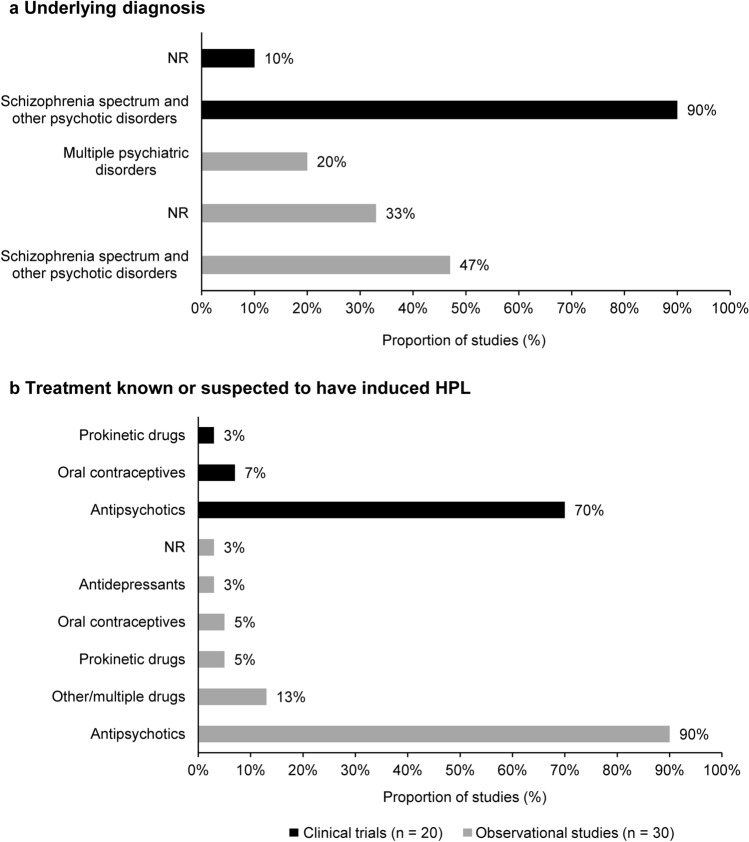
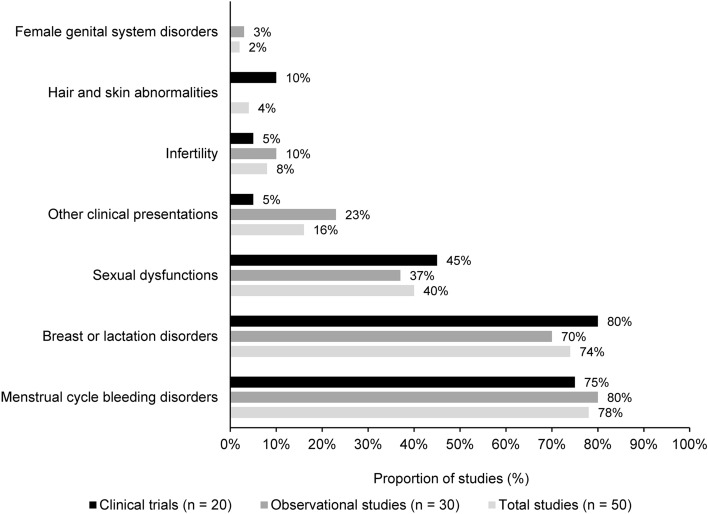
Screening for drug-induced hyperprolactinaemia, a condition characterised by higher-than-normal levels of serum prolactin induced by drug treatments, requires a comprehensive understanding of the clinical presentations and long-term complications of the condition. Using two databases, Embase and MEDLINE, we summarised the available evidence on the clinical presentations and long-term complications of drug-induced hyperprolactinaemia. Clinical and observational studies reporting on drug treatments known or suspected to induce hyperprolactinaemia were included. Database searches were limited to the English language; no date or geographic restrictions were applied. Fifty studies were identified for inclusion, comprising a variety of study designs and patient populations. Most data were reported in patients treated with antipsychotics, but symptoms were also described among patients receiving other drugs, such as prokinetic drugs and antidepressants. Notably, the diagnosis of drug-induced hyperprolactinaemia varied across studies since a standard definition of elevated prolactin levels was not consistently applied. Frequent clinical presentations of hyperprolactinaemia were menstrual cycle bleeding, breast or lactation disorders, and sexual dysfunctions, described in 80% (40/50), 74% (37/50), and 42% (21/50) of the included studies, respectively. In the few studies reporting such symptoms, the prevalence of vaginal dryness impacted up to 53% of females, and infertility in both sexes ranged from 15 to 31%. Clinicians should be aware of these symptoms related to drug-induced hyperprolactinaemia when treating patients with drugs that can alter prolactin levels. Future research should explore the long-term complications of drug-induced hyperprolactinaemia and apply accepted thresholds of elevated prolactin levels (i.e., 20 ng/mL for males and 25 ng/mL for females) to diagnose hyperprolactinaemia as a drug-induced adverse event.Trial Registration PROSPERO International Prospective Register Of Systematic Reviews (CRD42021245259).
© 2023. The Author(s).
Conflict of interest statement
DB is a current and SYH is a former employee of Takeda Development Center Americas, Inc. and received stock or stock options at the time of study. Currently SYH is employed by Ironwood Pharmaceuticals. DRJ and CCiC provide consultancy support to Takeda Development Center Americas, Inc. as employees of Evidera.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
