

Estimating COVID-19 vaccine uptake and its drivers among migrants, homeless and precariously housed people in France
- PMID: 36801917
- PMCID: PMC9939372
- DOI: 10.1038/s43856-023-00257-1
Estimating COVID-19 vaccine uptake and its drivers among migrants, homeless and precariously housed people in France
Abstract
Background: Migrants, people experiencing homelessness (PEH), or precariously housed (PH) are at high risk for COVID-19 infection, hospitalization, and death from COVID-19. However, while data on COVID-19 vaccine uptake in these populations are available in the USA, Canada, and Denmark, we are lacking, to the best of our knowledge, data from France.
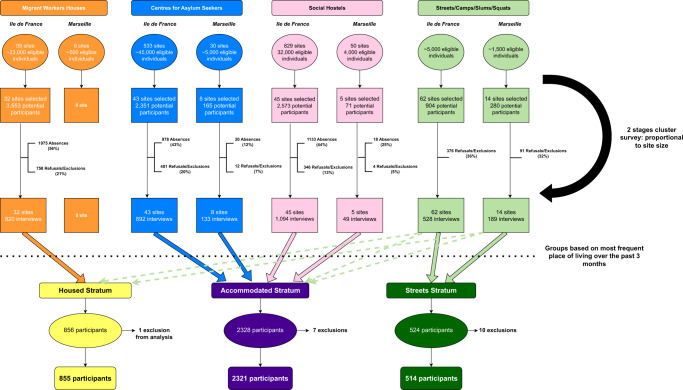
Methods: In late 2021, we carried out a cross-sectional survey to determine COVID-19 vaccine coverage in PEH/PH residing in Ile-de-France and Marseille, France, and to explore its drivers. Participants aged over 18 years were interviewed face-to-face where they slept the previous night, in their preferred language, and then stratified for analysis into three housing groups (Streets, Accommodated, and Precariously Housed). Standardized vaccination rates were computed and compared to the French population. Multilevel univariate and multivariable logistic regression models were built.
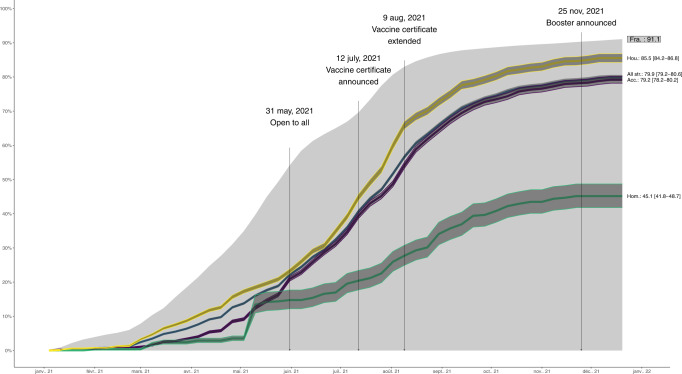
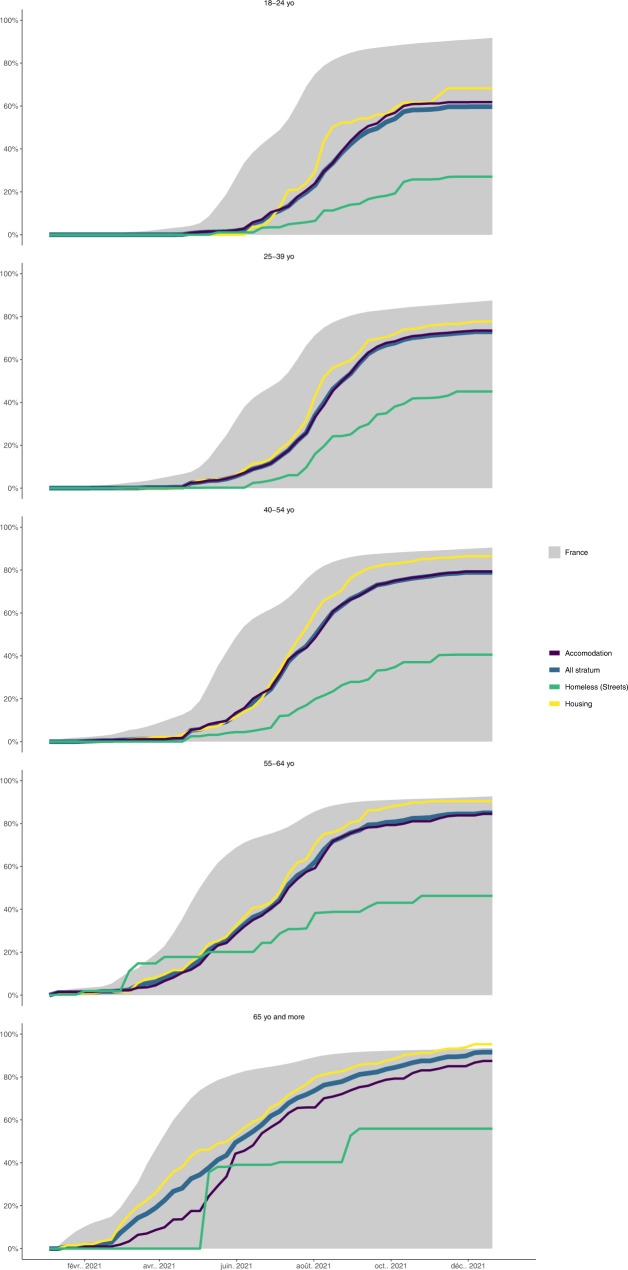
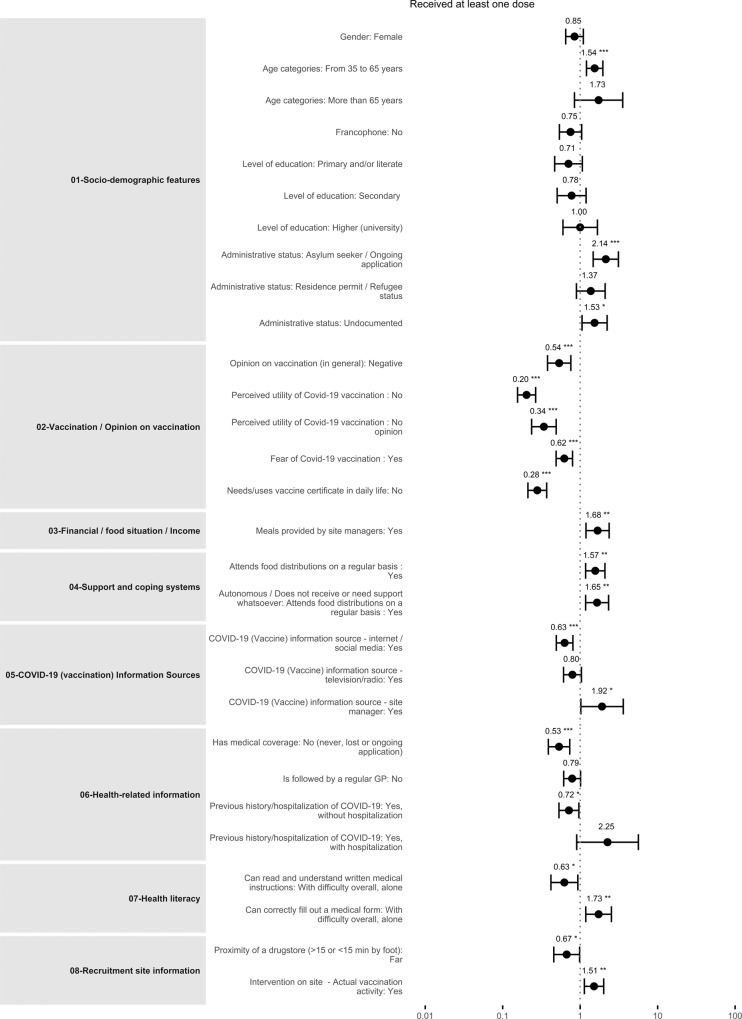
Results: We find that 76.2% (95% confidence interval [CI] 74.3-78.1) of the 3690 participants received at least one COVID-19 vaccine dose while 91.1% of the French population did so. Vaccine uptake varies by stratum, with the highest uptake (85.6%; reference) in PH, followed by Accommodated (75.4%; adjusted odds-ratio = 0.79; 95% CI 0.51-1.09 vs. PH) and lowest in Streets (42.0%; AOR = 0.38; 95%CI 0.25-0.57 vs. PH). Use for vaccine certificate, age, socioeconomic factors, and vaccine hesitancy is associated with vaccination coverage.
Conclusions: In France, PEH/PH, and especially the most excluded, are less likely than the general population to receive COVID-19 vaccines. While vaccine mandate has proved an effective strategy, targeted outreach, on-site vaccinations, and sensitization activities are strategies enhancing vaccine uptake that can easily be replicated in future campaigns and other settings.
Plain language summary
Vulnerable populations, such as people experiencing homelessness, are less likely to have a COVID-19 vaccine. We aimed to identify potential reasons for this, by interviewing homeless/precariously housed people in France. We found that although most homeless people have been vaccinated, vaccination rates are lower than the general population. Among the homeless, the least likely to be vaccinated are those living on the streets. The need for vaccine certificates and the support of social workers are positive drivers of vaccine uptake, while influence from family/friends, vaccine hesitancy and fear of the vaccine negatively affect uptake. Providing vaccines on-site and tailoring programs to better target these vulnerable groups should be priorities. Raising awareness by involving trusted third parties is also key to countering negative vaccine beliefs. Our insights apply beyond the COVID-19 crisis, when routinely supporting the health of vulnerable populations.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
COVID-19 vaccination uptake and receptivity among veterans enrolled in homelessness-tailored primary health care clinics: provider trust vs. misinformation.BMC Prim Care. 2024 Jan 12;25(1):24. doi: 10.1186/s12875-023-02251-x. BMC Prim Care. 2024. PMID: 38216894 Free PMC article.
-
COVID-19 vaccine coverage and factors associated with vaccine uptake among 23 247 adults with a recent history of homelessness in Ontario, Canada: a population-based cohort study.Lancet Public Health. 2022 Apr;7(4):e366-e377. doi: 10.1016/S2468-2667(22)00037-8. Epub 2022 Mar 9. Lancet Public Health. 2022. PMID: 35278362 Free PMC article.
-
Vaccine acceptance, determinants, and attitudes toward vaccine among people experiencing homelessness: a systematic review and meta-analysis.BMC Infect Dis. 2023 Dec 15;23(1):880. doi: 10.1186/s12879-023-08878-6. BMC Infect Dis. 2023. PMID: 38102542 Free PMC article.
-
Exploring COVID-19 vaccine uptake, confidence and hesitancy among people experiencing homelessness in Toronto, Canada: protocol for the Ku-gaa-gii pimitizi-win qualitative study.BMJ Open. 2022 Aug 17;12(8):e064225. doi: 10.1136/bmjopen-2022-064225. BMJ Open. 2022. PMID: 35977770 Free PMC article.
-
COVID-19 in the homeless population: a scoping review and meta-analysis examining differences in prevalence, presentation, vaccine hesitancy and government response in the first year of the pandemic.BMC Infect Dis. 2023 Mar 14;23(1):155. doi: 10.1186/s12879-023-08037-x. BMC Infect Dis. 2023. PMID: 36918758 Free PMC article.
Cited by
-
COVID-19 vaccination uptake and receptivity among veterans enrolled in homelessness-tailored primary health care clinics: provider trust vs. misinformation.BMC Prim Care. 2024 Jan 12;25(1):24. doi: 10.1186/s12875-023-02251-x. BMC Prim Care. 2024. PMID: 38216894 Free PMC article.
-
A systematic review and meta-analysis of the global prevalence and determinants of COVID-19 vaccine acceptance and uptake in people living with HIV.Nat Hum Behav. 2024 Jan;8(1):100-114. doi: 10.1038/s41562-023-01733-3. Epub 2023 Oct 30. Nat Hum Behav. 2024. PMID: 37904021 Free PMC article.
-
A conceptual framework to model social determinants of COVID-19 vaccination uptake among underserved homeless populations.Vaccine X. 2024 Mar 14;18:100472. doi: 10.1016/j.jvacx.2024.100472. eCollection 2024 Jun. Vaccine X. 2024. PMID: 38523621 Free PMC article.
-
Factors associated with the uptake of COVID-19 vaccination, testing and medical care among Myanmar migrants in Japan: a cross-sectional study.Trop Med Health. 2024 Aug 6;52(1):53. doi: 10.1186/s41182-024-00621-4. Trop Med Health. 2024. PMID: 39107852 Free PMC article.
-
A Mobile-Based Preventive Intervention for Young, Arabic-Speaking Asylum Seekers During the COVID-19 Pandemic in Germany: Design and Implementation.JMIR Form Res. 2023 Jun 5;7:e44551. doi: 10.2196/44551. JMIR Form Res. 2023. PMID: 37134019 Free PMC article.
References
LinkOut - more resources
Full Text Sources
