

Effects of Semaglutide on Albuminuria and Kidney Function in People With Overweight or Obesity With or Without Type 2 Diabetes: Exploratory Analysis From the STEP 1, 2, and 3 Trials
- PMID: 36801984
- PMCID: PMC10090901
- DOI: 10.2337/dc22-1889
Effects of Semaglutide on Albuminuria and Kidney Function in People With Overweight or Obesity With or Without Type 2 Diabetes: Exploratory Analysis From the STEP 1, 2, and 3 Trials
Abstract
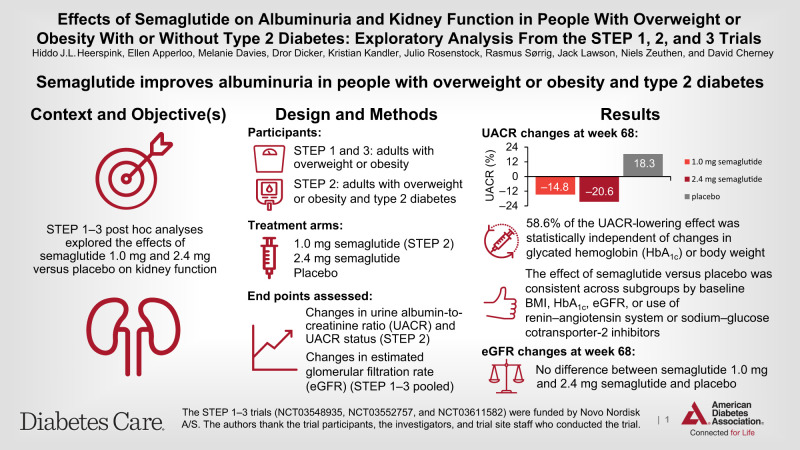
Objective: These post hoc analyses of the Semaglutide Treatment Effect in People with obesity (STEP) 1-3 trials (NCT03548935, NCT03552757, and NCT03611582) explored the effects of semaglutide (up to 2.4 mg) on kidney function.
Research design and methods: STEP 1-3 included adults with overweight/obesity; STEP 2 patients also had type 2 diabetes. Participants received once-weekly subcutaneous semaglutide 1.0 mg (STEP 2 only), 2.4 mg, or placebo for 68 weeks, plus lifestyle intervention (STEP 1 and 2) or intensive behavioral therapy (STEP 3). Changes in urine albumin-to-creatinine ratio (UACR) and UACR status from baseline to week 68 were assessed for STEP 2. Changes in estimated glomerular filtration rate (eGFR) were assessed from pooled STEP 1-3 data.
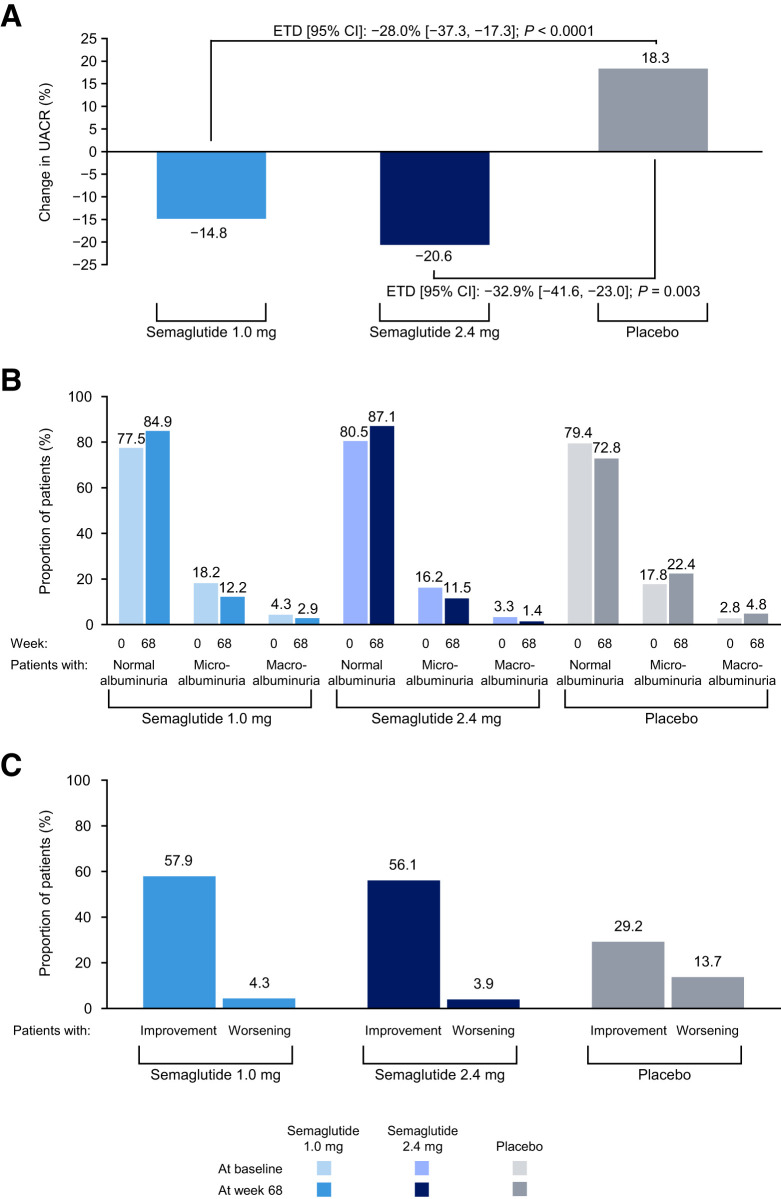
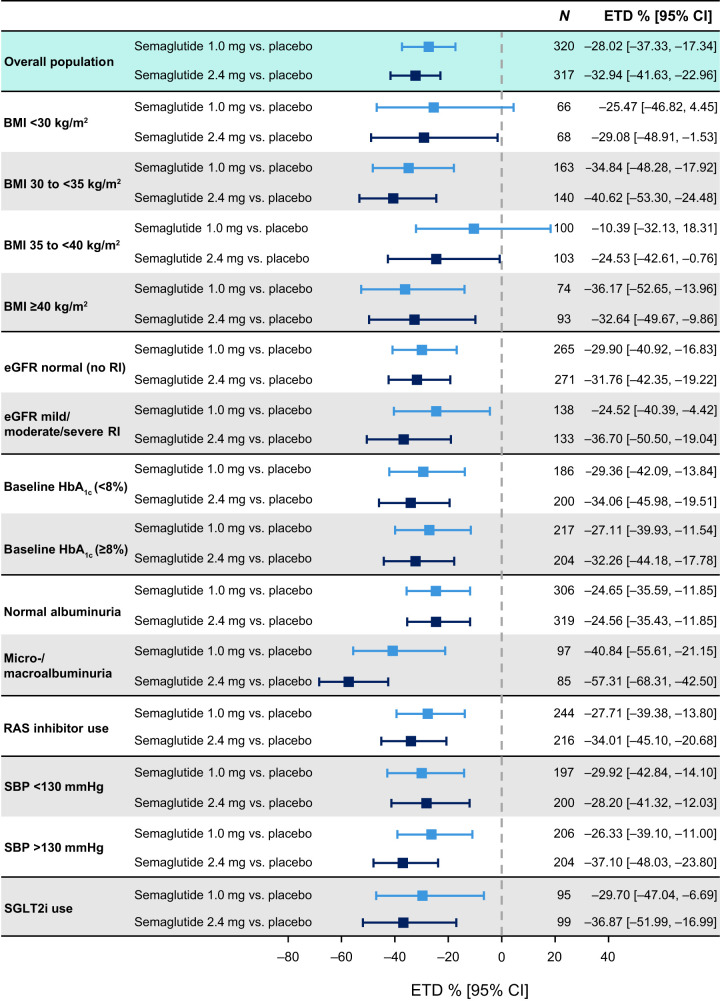
Results: In STEP 2, 1,205 (99.6% total cohort) patients had UACR data; geometric mean baseline UACR was 13.7, 12.5, and 13.2 mg/g with semaglutide 1.0 mg, 2.4 mg, and placebo, respectively. At week 68, UACR changes were -14.8% and -20.6% with semaglutide 1.0 mg and 2.4 mg, respectively, and +18.3% with placebo (between-group differences [95% CI] vs. placebo: -28.0% [-37.3, -17.3], P < 0.0001 for semaglutide 1.0 mg; -32.9% [-41.6, -23.0], P = 0.003 for semaglutide 2.4 mg). UACR status improved in greater proportions of patients with semaglutide 1.0 mg and 2.4 mg versus placebo (P = 0.0004 and P = 0.0014, respectively). In the pooled STEP 1-3 analyses, 3,379 participants had eGFR data; there was no difference between semaglutide 2.4 mg and placebo in eGFR trajectories at week 68.
Conclusions: Semaglutide improved UACR in adults with overweight/obesity and type 2 diabetes. In participants with normal kidney function, semaglutide did not have an effect on eGFR decline.
© 2023 by the American Diabetes Association.
Conflict of interest statement
Figures
References
-
- de Boer IH, Caramori ML, Chan JCN, et al. Executive summary of the 2020 KDIGO Diabetes Management in CKD Guideline: evidence-based advances in monitoring and treatment. Kidney Int 2020;98:839–848 - PubMed
-
- American Diabetes Association Professional Practice Committee . 8. Obesity and weight management for the prevention and treatment of type 2 diabetes: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022;45(Suppl. 1):S113–S124 - PubMed
-
- Sharma M. The RENAAL study investigation. Clin Diabetes 2002;20:19–20
-
- Rodby RA, Rohde RD, Clarke WR, et al.; Collaborative Study Group . The Irbesartan Type II Diabetic Nephropathy Trial: study design and baseline patient characteristics. Nephrol Dial Transplant 2000;15:487–497 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
