

Prevention of incisional surgical site infection by subfascial closed suction drainage after open laparotomy: a single surgeon experience in 250 consecutive patients
- PMID: 36803411
- PMCID: PMC9942376
- DOI: 10.1186/s13037-023-00354-z
Prevention of incisional surgical site infection by subfascial closed suction drainage after open laparotomy: a single surgeon experience in 250 consecutive patients
Abstract
Background: Open laparotomy with gastroenterological surgery is a surgical procedure results in a relatively high rate (about 10% or more) of incisional surgical site infection (SSI). To reduce incisional SSI after open laparotomy, mechanical preventors, such as subcutaneous wound drainage or negative-pressure wound therapy (NPWT), have been tried; however, conclusive results have not been obtained. This study evaluated the prevention of incisional SSI by first subfascial closed suction drainage after open laparotomy.
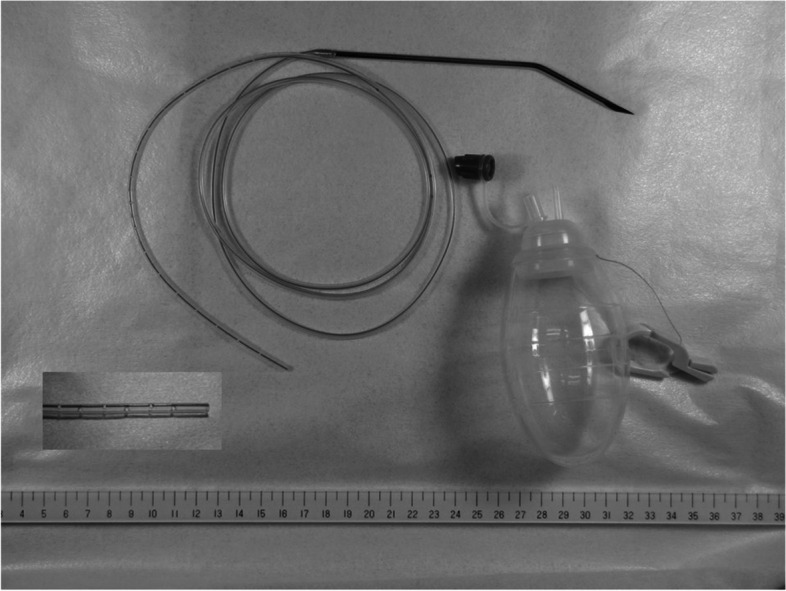
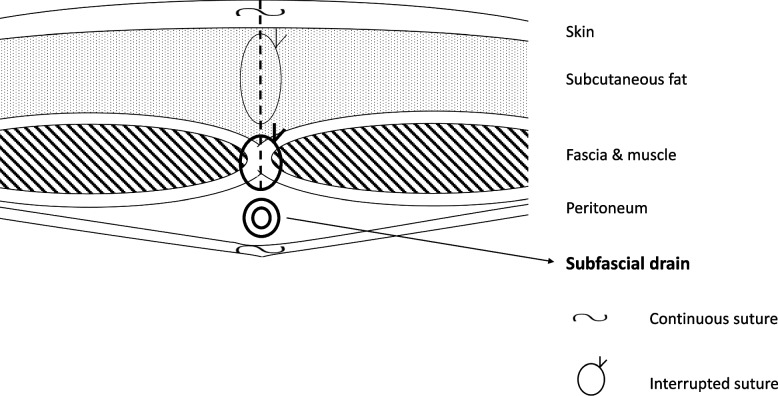
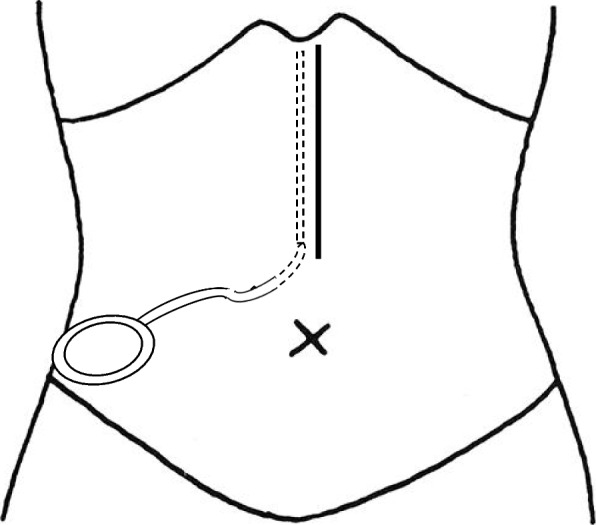
Methods: A total of 453 consecutive patients who underwent open laparotomy with gastroenterological surgery by one surgeon in one hospital (between August 1, 2011, and August 31, 2022) was investigated. Same absorbable threads and ring drapes were used in this period. Subfascial drainage was used in consecutive 250 patients in the later period (between January 1, 2016, and August 31, 2022). The incidences of SSIs in the subfascial drainage group were compared to those of in the no subfascial drainage group.
Results: (a) No incisional SSI (superficial and deep) occurred in the subfascial drainage group (superficial = 0% [0/250] and deep = 0% [0/250]). As a result, incidences of incisional SSI of the subfascial drainage group were significantly lower than those of the no subfascial drainage group (superficial = 8.9% [18/203]; deep = 3.4% [7/203]) (p < 0.001 and p = 0.003, respectively). (b) Four out of seven deep incisional SSI patients in the no subfascial drainage group underwent debridement and re-suture under lumbar or general anesthesia. (c) There was no significant difference in the incidences of organ/space SSI of the two groups (3.4% [7/203] in the no subfascial drainage group and 5.2% [13/250] in the subfascial drainage group) (P = 0.491).
Conclusion: Subfascial drainage was associated with no incisional SSI after open laparotomy with gastroenterological surgery.
Keywords: Gastroenterological surgery; Incisional surgical site infection; Laparotomy; Subfascial closed suction drainage; Surgical site infection.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
A combination of subcuticular sutures and subcutaneous closed-suction drainage reduces the risk of incisional surgical site infection in loop ileostomy closure.Surg Today. 2021 Apr;51(4):605-611. doi: 10.1007/s00595-020-02128-x. Epub 2020 Sep 4. Surg Today. 2021. PMID: 32888080
-
Combined Incisional Negative Pressure Wound Therapy and Subfascial Suction Drainage: The Suction Taco Approach.Cureus. 2023 Aug 16;15(8):e43577. doi: 10.7759/cureus.43577. eCollection 2023 Aug. Cureus. 2023. PMID: 37719597 Free PMC article.
-
Phase II Randomized Trial of Negative-Pressure Wound Therapy to Decrease Surgical Site Infection in Patients Undergoing Laparotomy for Gastrointestinal, Pancreatic, and Peritoneal Surface Malignancies.J Am Coll Surg. 2017 Apr;224(4):726-737. doi: 10.1016/j.jamcollsurg.2016.12.028. Epub 2017 Jan 11. J Am Coll Surg. 2017. PMID: 28088597 Free PMC article. Clinical Trial.
-
Prophylactic negative pressure wound therapy for closed laparotomy wounds: a systematic review and meta-analysis of randomised controlled trials.Ir J Med Sci. 2021 Feb;190(1):261-267. doi: 10.1007/s11845-020-02283-7. Epub 2020 Jun 25. Ir J Med Sci. 2021. PMID: 32588378 Free PMC article.
-
Negative Pressure Wound Therapy for Closed Laparotomy Incisions in General and Colorectal Surgery: A Systematic Review and Meta-analysis.JAMA Surg. 2018 Nov 1;153(11):e183467. doi: 10.1001/jamasurg.2018.3467. Epub 2018 Nov 21. JAMA Surg. 2018. PMID: 30267040 Free PMC article.
Cited by
-
A meta-analysis of the risk factors for surgical site infection in patients with colorectal cancer.Int Wound J. 2023 Oct 31;21(2):e14459. doi: 10.1111/iwj.14459. Online ahead of print. Int Wound J. 2023. Retraction in: Int Wound J. 2025 Mar;22(3):e70266. doi: 10.1111/iwj.70266. PMID: 37904719 Free PMC article. Retracted.
References
LinkOut - more resources
Full Text Sources
Research Materials
